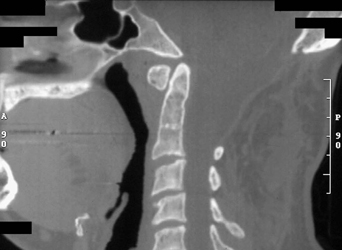
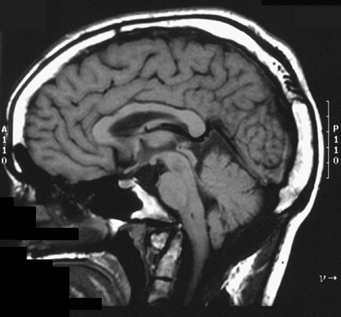
17 A 30-year-old man had a previous suboccipital craniectomy for Chiari I malformation, with C1–C3 laminectomies. Postoperatively, he had intractable progressive neck pain. On examination, he had brisk reflexes, upgoing toes, and a jaw jerk. Sagittal computed tomography (CT) reconstruction of the occipitocervical junction shows a segmentation abnormality with C2–C3 autofusion, the previous occipitocervical decompression, and cranial settling (Fig. 17-1). Sagittal brain magnetic resonance imaging (MRI) features more prominently the invagination of the brainstem and platybasia (Fig. 17-2). FIGURE 17-1 Sagittal CT reconstruction of the occipitocervical junction shows an abnormally elongated C2, the previous occipitocervical decompression, and cranial settling. Vertical subluxation of C2 with platybasia An occipitocervical fusion was accomplished with rib graft (Fig. 17-3).
Cranial Settling
Presentation
Radiologic Findings
Diagnosis
Treatment
Cranial Settling
Only gold members can continue reading. Log In or Register to continue







Full access? Get Clinical Tree


