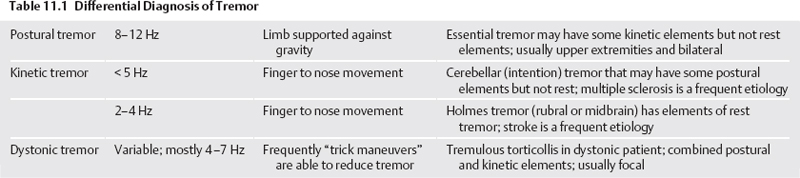
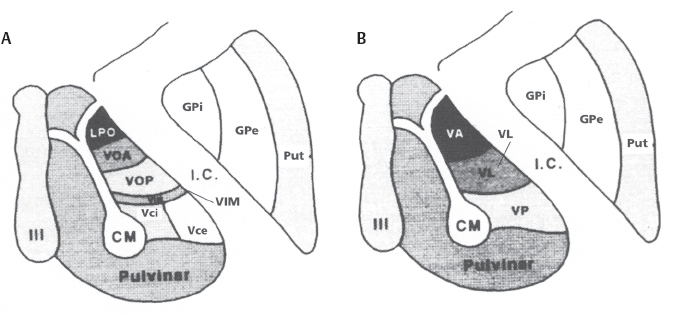
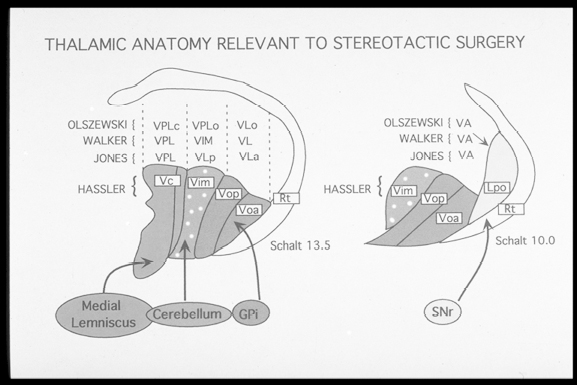
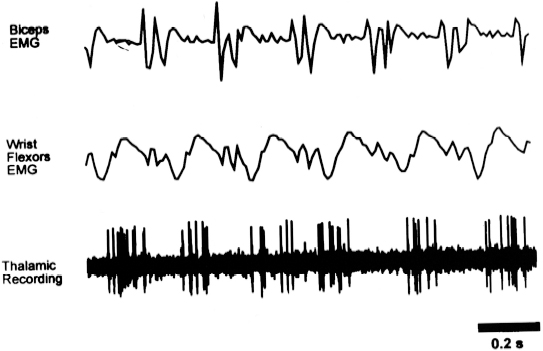
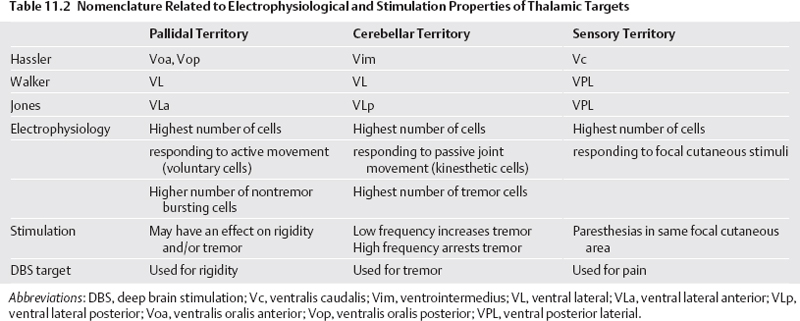
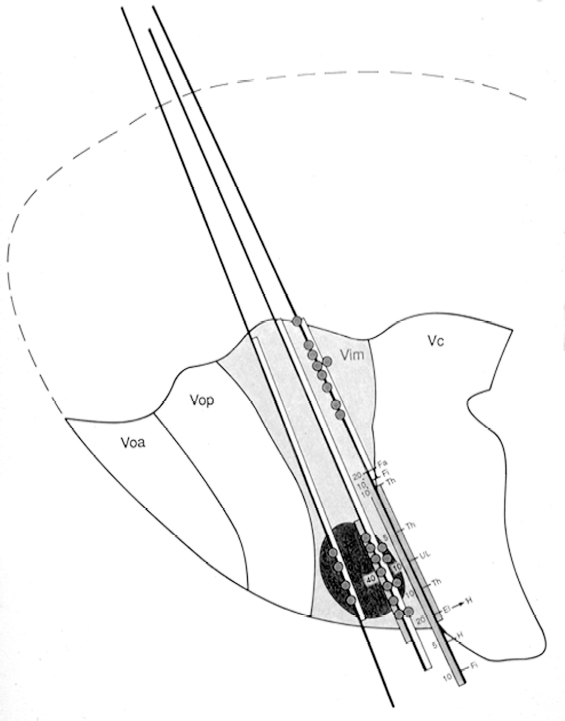
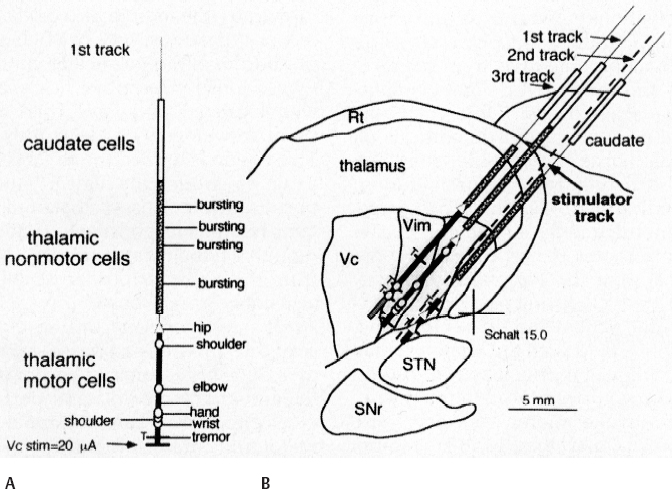
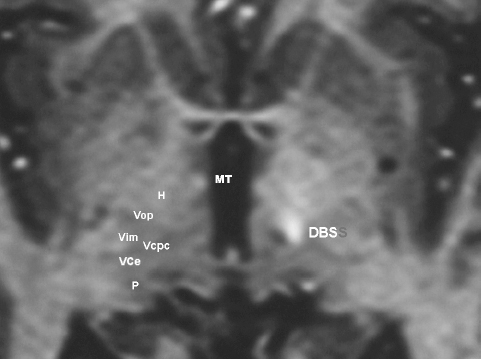
11 Deep Brain Stimulation for Tremor Jorge L. Eller and Kim J. Burchiel Tremor is the most prevalent of the movement disorders and is defined as an involuntary, rhythmic, oscillatory contraction of agonist and antagonist muscles that exhibits a regular frequency. Tremor is further categorized as rest or action (postural, kinetic tremor, task-specific, etc.), depending on when it occurs.1 Resting tremor is defined as tremor occurring in an extremity fully supported against gravity. Postural tremor is defined as tremor occurring when the extremity is maintaining position against gravity. Kinetic (the preferred term over intentional) tremor is defined as tremor occurring with voluntary movement from one point in space to another. Task-specific tremor describes tremor that increases in amplitude during movement directed at a particular goal (e.g., writing tremor). Moreover, tremor can be further characterized objectively with electromyography, accelerometry, and Fourier analysis.2,3 The differential diagnosis of tremor divides it into specific clinical entities, the most common being essential tremor (ET), parkinsonian tremor, cerebellar outflow tremor, Holmes tremor (also called rubral tremor), and dystonic tremor (Table 11.1). These can be differentiated based upon features in the history and physical exam as well as electrophysiological characteristics.4 Epidemiological studies of ET confirm that it is the most common movement disorder. A 45-year retrospective analysis of medical records from Rochester, Minnesota, revealed the incidence and prevalence of ET were 23.7 and 305.6 per 100,000 cases, respectively. Mean age of diagnosis was 58 years, with men and women being equally affected. The investigators noted that age-specific incidence increased after 49 years of age and peaked in the 80s.5–7 Although a gene variant (HS1-BP3) on chromosome 2 is associated with familiar ET, the pathophysiology of ET remains unknown. No obvious histopathologic abnormalities are associated with ET; therefore, no animal models are available that conclusively replicate human ET. An aberrant central oscillator in the inferior olive is hypothesized as one possible cause of ET. The rationale is that the olivocerebellar oscillations are transmitted via the cerebellothalamocortical pathway, thus encompassing the cerebellum, thalamus, and brainstem areas that are known to be involved in ET.8,9 The early days of functional neurosurgery involved destruction of parts of the motor system.10–12 Surgery to treat movement disorders became popular following Spiegel and Wycis’s 1947 development of the first stereotactic apparatus that enabled minimally invasive surgery on deep nuclei in the human brain.12 Further refinement eventually led to the determination that Hassler’s ventrointermedius (Vim) nucleus of the thalamus is the optimal surgical target (Fig. 11.1). Regardless of tremor etiology, Vim is the preferred target of surgery to treat tremor except dystonic tremor (see Chapter 12) and of course psychogenic tremor. The Vim is the major termination of cerebellar efferents of the cerebellothalamocortical pathway (Fig. 11.2) and projects to the motor cortex.14 This area contains the greatest concentration of tremor cells or neurons that fire in bursts synchronous with the patient’s tremor (Fig. 11.3). In addition to the anatomical connection revealed in primate tracing studies, positron emission tomography (PET) has demonstrated an increase in blood flow to the ipsilateral motor cortex with stimulation of the thalamic Vim, suggesting a functional connection between these structures.15 The surgical repertoire available to treat tremor includes either ablation of the contralateral thalamic Vim by means of radiofrequency lesion (thalamotomy) or placement of a deep brain stimulation (DBS) electrode in the contralateral thalamic Vim. In 1991, Benabid et al published an article that described tremor suppression with chronic high-frequency stimulation of the thalamic Vim nucleus.16 Although it had been known since the 1950s that high-frequency stimulation of the Vim nucleus could arrest tremor acutely, this introduced the first practical technique for chronic brain stimulation as an alternative to lesioning (thalamotomy) in the treatment of tremor. Indications for both procedures are similar. Basically, patients must have tremor that is refractory to medical therapy and represents the predominant manifestation of the disorder. The ideal candidates for thalamic surgery are patients with ET and those with tremor-predominant Parkinson disease (PD), although surgery may also be considered for tremor secondary to multiple sclerosis, stroke, or trauma. The remainder of this chapter describes our surgical technique and experience with placement of DBS electrodes to treat tremor. Fig. 11.1 Terminology of the thalamic nuclei. (A) Hassler classification system. (B) Anglo-American classification system. LPO, lateral polaris; VOA, ventral oral anterior; VOP, ventral oral posterior; VIM, ventral intermediate; Vci, ventral caudal internal; Vce, ventral caudal external; CM, centrum medianum; VA, ventral anterior; VL, ventral lateral; VP, ventral posterior; GPi, internal segment of the globus pallidus; GPe, external segment of the globus pallidus; put, putamen; I.C., intercommissural region; III, third ventricle. (From Burchiel KJ. Thalamotomy for movement disorders. Neurosurg Clin N Am 1995;6:55–71.) Fig. 11.2 Thalamic neuroanatomy relevant to neurosurgery. The major inputs to the sensory and motor thalamus are illustrated using Hassler’s nomenclature and alternative nomenclature. The ventral lateral (VL) nucleus is roughly the equivalent of Hassler’s nucleus ventralis oralis anterior (Voa), nucleus ventrali oralis posterior (Vop), and ventral intermediate (Vim). Vim receives both vestibulothalamic and cerebellothalamic afferents. Vop may also receive cerebellothalamic afferents. Both Vop and Voa receive pallidothalamic fibers from the medial globus pallidus interna (Gpi). Fig. 11.3 Tremor cells recorded from the VIM (bottom). Note the correlation between the neuronal discharges from the tremor cells and the electromyogram. These discharges stop when the tremor ceases. (Modified from Bakay RAE, Vitek JL, Delong MR. Thalamotomy for tremor. In: Rengechary SS, Wilkins RR, eds. Neurosurgical Operative Atlas. Vol 2. Park Ridge, IL: American Association of Neurological Surgeons; 1992:299–312.) The Walker nomenclature of the ventral lateral (VL) thalamus is less precise than the Hassler terminology (Table 11.2). The VL nucleus is roughly the equivalent of Hassler’s nucleus ventralis oralis anterior (Voa), nucleus ventralis oralis posterior (Vop), and Vim. Vim receives both vestibulo-thalamic and cerebellothalamic afferents and projects to the primary motor cortex (area 4) but not to area 3a of the sensorimotor cortex as suggested by Hassler. Vop may also receive cerebellothalamic afferents. Both Vop and Voa receive pallidothalamic fibers from the medial globus pallidus (GPi), and project to the precentral motor cortex and the supplementary motor cortex. Empirically, lesioning of the Voa/Vop is considered a target for control of rigidity and dyskinesia, whereas Vim is the best target for control of tremor. Despite multiple attempts to modify Hassler’s nomenclature to a more contemporary and accurate reflection of the neuroanatomy, functional neurosurgeons have kept it because the sensory and motor subdivisions matched what has been observed anatomically, electrophysiologically, and physiologically.17 These subnuclei are differentiated electrophysiologically (Fig. 11.4). Although most neurons in Vop and Vim fire in the 10 to 20 Hz range, there are tremor-synchronous neurons with rhythmic 5 to 7 Hz bursts. These tremor cells are recorded primarily in Vim, and to a limited extent in Vop. In PD, these tremor cells occur approximately four times as often as in ET and five times more often than in Holmes or cerebellar tremors.18 The highest percentage of nontremor bursting neurons occurs in Vop, but also occurs frequently in Voa. Neurons that alter their firing rate with joint movement or deep muscle pressure are called kinesthetic cells. These are very common in Vim (44%), but uncommon in Vop (16%),19 whereas neurons that change their firing rate with active movements are called voluntary cells and are common in Vop (70%) and less so in Vim (49%), but are rare in Voa. When transitioning into the thalamic sensory ventralis caudalis nucleus (Vc), there is a “shell” of deep sensory (proprioceptive) neurons (Vcae) that respond to deep pressure (66%) prior to the cutaneous responsive neurons (Vcpe).20 Identifying these subdivisions then facilitates lead placement (Fig. 11.5). There are multiple potential targets for DBS to affect tremor, including the pallidothalamic cells in the GPi,21,22 the point where the pallidal and cerebellar fibers cross the subthalamic area around the zona incerta, the fields of Forel (subthalamic lesion or campotomy),23–25 at their termination in Vim,26–42 or downstream projections to the GPi from the subthalamic nucleus (STN).21,22,43,44 Vim DBS is currently believed to be the best procedure for treating all forms of tremor and is the focus of this chapter. There have been several optimal thalamic locations for tremor suppression described in the past: anterior to where evoked potentials can be recorded in response to cutaneous stimulation of the thumb,45 where there are hand kinesthetic cells and where electrical stimulation produces effects on tremor,46 where electrical stimulation effects tremor and anterior to where electrical stimulation evokes sensations,47 or where there is tremor cell activity.48 These all appear to describe the same site. However, the optimal thalamic DBS site may be more anterior and dorsal49 and is probably more medial50 (i.e., the Vim/Vop boarder). DBS stimulation, unlike lesioning, alters the characteristics of the tremor.51–53 PET consistently demonstrates Vim DBS tremor suppression is associated with decreased regional blood flow in multiple ipsilateral motor-related cortical and cerebellar areas suggesting modulation of the cerebellothalamocortical pathways.11,54 Where the tremor (pathological or physiological) originates is unknown. The focus of stereotactic surgeons in the past was primarily on tremor, especially parkinsonian tremor. Tremor, however, is usually not the most disabling symptom of PD. Akinesia is the most disabling feature of the disease and is not ameliorated by Vim DBS. The combination of both resting and intention tremors is not uncommon in severely affected PD patients and is likely to be disabling. However, at this point in the disease process, the other symptoms of PD often require treatment and would likely be better treated with stimulation of the STN or GPi. Reevaluation of appropriate targets has led to targeting of the STN or GPi more commonly to treat parkinsonian akinesia, rigidity, and gait disturbance of PD in addition to the tremor. Thalamotomy remains an option in the treatment of tremor for well-informed patients who decide against stimulation, in cases where DBS fails, where the cost is prohibitive, or in remote areas where mandatory follow-up for adjustments of pulse generators is not possible.55 However, there are very few comparative studies and little randomized data upon which to scientifically base clinical practice.29,33,38 Fig. 11.4 Three representative microelectrode tracts through the ventrolateral thalamus. The labeled nuclei are ventralis oralis anterior (Voa), ventralis oralis posterior (Vop), ventrointermedius (Vim), and ventralis caudalis (Vc). The electrode tracts are depicted by the three straight lines entering the thalamus from the anterodorsal border and proceeding in a caudoventral direction. Neurons were isolated using standard electrophysiological techniques, and the sensory modality and somatotopic specificity were assessed for each neuron. Neuronal responses to somatosensory examination are coded by letters depicting the body part and the color of the bar along the right side to the electrode tract, which depicts the sensory modality. Portions of the tract in which tactile responses were found are in green; those with deep proprioceptive responses are colored yellow. Body regions are depicted by the letter along the right side of the tract: El, elbow; Fa, face; Fi, finger; H, hand; L, leg; M, mouth; S, shoulder; Th, thumb; UL, upper lip; W, wrist. Along the left side of the tract, the purple bar depicts the response to microstimulation; the numbers are the thresholds in microamps required to elicit a sensory response. The solid red circles denote cells with a tremor-related firing pattern. The shaded region encompasses the greatest concentration of tremor-related cells found in the ventral portion of the Vim. The penetrations through the thalamus in this orientation in the parasagittal plane generally proceed through the leg area into the arm area. Proximal limb regions are encountered before distal limb regions (e.g., shoulder regions are encountered first, followed by progressively more distal arm regions). The relatively greater number of neuronal responses related to the arm and face area reflect the somatotopic organization (homunculus) in the Vim with face, arm, and leg areas oriented in a medial-to-lateral direction. Deep pressure responses are found through the Vim, giving way to tactile responses as one proceeds into the Vc. Responses to microstimulation are generally similar to those found on somatosensory examination; the thresholds decrease as one moves closer toward the Vc. For patients with other types of disabling tremor, thalamic stimulation remains a viable option. Approximately a third of ET patients will be refractory to medical therapy and are potential candidates for thalamic stimulation. There is no effective medication for cerebellar or Holmes tremors. These result from several etiologies, including multiple sclerosis, stroke, or head injury. Nevertheless, all of these pathological tremors may respond to some degree to thalamic stimulation. These patients must be evaluated very carefully because damage to the brain may result in a less predictable surgical result. Surgical success is diminished and the risk of complications increased in the presence of severe generalized brain atrophy, ataxia, and significant memory or speech abnormalities. If the tremor is unilateral or dramatically asymmetrical, the surgical recommendation is straightforward. If the tremor is bilateral but asymmetrical, there is more uncertainty as to the most effective method of treatment. Some stereotactic neurosurgeons would prefer treating the more severely affected side and hope postoperatively that medications will optimize the effectiveness. Others would concentrate on the dominant side to allow maximum rehabilitation from a unilateral procedure. In our opinion, the best choice depends on the degree of asymmetry. Patients with dramatic differences in side-to-side tremor should be operated on the more severely affected side. In those where asymmetry is less marked, we prefer operating on the dominant hemisphere to restore function to the dominant side. If the patient has symmetrical bilateral tremor, there is again less controversy, with the dominant side being operated on first to provide a unilateral procedure, which would be functionally beneficial. If at all possible, a second procedure should be avoided because the risk of complications increases, even with DBS. When a second-side procedure is unavoidable due to the severity of the symptoms, then we prefer to wait 3 to 6 months before the second side is operated upon. This will ensure that the second operation is necessary and allows one to better assess the potential for complications. Fig. 11.5 Method of microelectrode mapping of the motor and sensory thalamus before placement of a stimulator for essential tremor. Segments of the track reconstructions are shaded to indicate caudate cells (open segment), nonmotor thalamus (stippled segment), motor thalamus (black segment), or sensory thalamus (gray segment). Locations of movement-related cells are indicated by triangles (leg), or circles (arm). (A) Detail of the first microelectrode track. The microstimulation threshold for sensory activation, marked “Vc stim,” was measured at the bottom of this track (frequency = 300 Hz, pulse width = 200 μs). (B) Three microelectrode tracks are superimposed on a scaled map of the thalamus and basal ganglia in a parasagittal plane (Schaltenbrand and Bailey Atlas parasagittal 15 plane) according to the surgical team’s judgment of the best fit of the tracks to the atlas. As illustrated here, the fit of actual micro-electrode tracks to a standard atlas map is frequently not perfect. The eventual location of the stimulator is shown as a dotted line. (Starr PA, Vitek JL, Bakay RAE. Deep brain stimulation for movement disorders. Neurosurg Clin N Am 1998;9:381–402.) The surgical implantation of DBS electrodes involves sequential steps, and optimal results require careful performance. Placement of a stereotactic frame is the first step and sets the stage for magnetic resonance imaging (MRI)-guided stereotactic localization. At our institution, we use the Leksell Stereotactic System (Elekta Inc., Norcross, GA, www.elekta.com/healthcareus.nsf). To obtain images that easily correlate with standard brain neuroanatomical atlases, this frame requires placement orthogonal to the anatomical planes of the brain. The frame has ear bars to prevent lateral tilt or rotation. The anteroposterior axis of the frame should be placed parallel to a line connecting the glabela to the inion, which places the frame parallel to the anterior commissure–posterior commissure (AC–PC) line.56 Anatomical targeting of the Vim is the next step and employs a combination of indirect and direct targeting. Indirect targeting is based upon fixed distances from the midpoint of a line connecting the AC to the PC to the Vim nucleus. The locations of the AC and PC can be determined by MRI, CT, or ventriculography. MRI is slightly less accurate than CT, with average errors of ~2 mm due to artifacts related to inhomogeneities in the magnetic field. In an attempt to decrease such errors, imaging fusion, or overlapping of CT and MRI data, is often used.57–59 Targeting of the Vim nucleus is then accomplished with the use of computer programs such as the FrameLink Stereotactic Linking System software (Medtronic Neuro Navigation, Louisville, CO, www.MedtronicNavigation.com) that relate a standard atlas10 to the patient’s radiological anatomy, as measured by CT or MRI.60 In this manner the radiological location of the Vim nucleus is converted to Cartesian coordinates on the Leksell frame. In an attempt to compensate for individual variations in nuclear location, direct targeting is based upon direct visualization of nuclear boundaries in an MRI T2 fast spin echo (FSE) sequence. Unfortunately, it is not always possible to clearly visualize target borders in MRI sequences. The patient is brought to the operating room and positioned supine, with the head slightly elevated. The Leksell frame is fixated to the Mayfield headholder with an adapter. Standard prepping and draping are performed and local anesthetic injected. A single bifrontal semicurve C-shaped incision is performed, anterior to the coronal suture. Burr holes are placed anterior to the coronal suture and 2.5 cm from the midline on either side. Dura and pia are coagulated and opened sharply. The Leksell arc is positioned for a standard trajectory of 60 degrees from the AC–PC line. Due to limitations inherent to mechanical properties of the stereotactic frame and the imaging technique employed, anatomical targeting alone is insufficient for optimal electrode placement. Standard stereotactic frame system precision has been measured to be approximately within 1.5 mm (95% confidence interval).61 Furthermore, MRI distortion effects, imperfect visualization of the anatomical target, potential brain shift, and variability of physiological function within any specific anatomical target further decrease the accuracy of anatomical targeting.62 Therefore, physiological methods for localization are important to confirm and if necessary adjust the final placement of the DBS lead. Two physiological methods to refine anatomical targeting are microelectrode recording (MER) and macrostimulation. MER isolates single neuronal action potentials using platinumiridium or tungsten microelectrodes with an impedance greater than 500 KΩ.63,64 The microelectrode is attached to a microdrive and mounted on the stereotactic frame. The microelectrode tip is retracted into a protective cylindrical sheath and inserted to a standard depth, from which the microdrive is used to drive the microelectrode toward the target,65 and the signal from the microelectrode is amplified and filtered. Neuronal discharges are viewed on an oscilloscope and sound is heard through an audio monitor. Distinguishing characteristic patterns of spontaneous discharge within the nuclei of the basal ganglia are then used for localization. Macrostimulation is employed to identify the target area in the Vim nucleus by a high-frequency stimulation-evoked decrease in tremor. Similarly macrostimulation can be used to identify the internal capsule (by stimulation-evoked contractions of skeletal muscle), and the thalamic sensory ventralis caudalis (Vc) nucleus (by stimulation-evoked paresthesias). At our institution, once the target is defined bilaterally using anatomical and physiological techniques, we proceed to implant the DBS leads. There are two US Food and Drug Administration (FDA)-approved lead models (Medtronic Minneapolis, MN, www.medtronic.com/physician/activa/techmanuals.html). Both are quadripolar with four platinumiridium contacts at the distal end. Each contact is 1.5 mm in length and separated by wide (1.5 mm) spacing (model #3387) or narrow (0.5 mm) spacing (model #3389). The lead is implanted along the desired MER trajectory with the second contact from the tip (#1 contact) positioned at the target. The lead is then secured in place using the Stimloc ring and cap lead anchor system (Medtronic, Inc., Minneapolis, MN). Intraoperative lateral fluoroscopy is used to confirm that the DBS lead remains in position after being detached from the stereotactic frame and secured in the Stimloc device. The procedure is repeated for the DBS lead on the other side. The DBS leads are then tunneled under the subgaleal tissue, and the surgical wound is closed with special care to avoid damaging the leads. The stereotactic Leksell frame is then removed. To finalize the procedure the patient is placed under general anesthesia, positioned supine with the head turned away from the side of the implant. An internal pulse generator (IPG) is usually placed in a subcutaneous pocket below the clavicle. Therefore, the bifrontal incision, as well as the ipsilateral retroauricular, cervical, and subclavicular areas, are prepped and draped in sterile fashion. To accommodate the IPG an incision is performed 2.5 cm below the clavicle, and a subcutaneous pocket is created over the pectoralis fascia. A second incision is created 2.5 cm posterior to the ipsilateral ear for placement of the connectors between the distal ends of the DBS leads and the extension cables that will connect the DBS leads to the IPG. Care is taken to assure that these connectors will sit over the periosteum, in a sub-galeal pocket created to accommodate them, and not in the neck, where excessive movement may cause lead fracture. The extension cables are tunneled from the subclavicular pocket to the retroauricular incision. In a similar fashion, the distal ends of the DBS leads are retrieved and tunneled from the bifrontal incision (which is reopened carefully so as not to damage the leads) to the retroauricular incision. The DBS leads are connected to the extension cables using a standard four-screw connector, which is protected by a Silastic (Dow Corning, Midland, MI) sheath and placed in the subgaleal pocket mentioned earlier. The distal ends of the extension cables are then connected to the IPG. All wounds are irrigated with antibiotic irrigation and closed in layers. The DBS IPG is programmed using an external programming device. Adjustable stimulation variables include amplitude, frequency, pulse width, and choice of active contacts (see Chapter 13). Editor’s Comments For initial target coordinates for stereotactic procedures, we use serial 1.5 mm contiguous, nonoverlapping, contrast-enhanced three-dimensional (3D) volumetric 1.5T MRI studies,66 which are performed through the entire brain (for our technique see Chapter 7). Direct identification of the Vim target remains very difficult but possible on occasion (Fig. 11.6). Use of planning stations allows calculation not only of the target but also of the entry point and trajectory to the target. Contrast allows cortical veins to be easily visualized, and trajectories can be customized for each patient to avoid deep blood vessels in the ventricle en route to the desired target. Many times, the ventricular system may be avoided as well by choosing a more lateral entry point. Proponents of this technique argue that penetration of the ventricular system causes increased brain shift due to excess cerebrospinal fluid (CSF) loss, potential damage to blood vessels, and alteration of microelectrode trajectory by passing through matter of variable densities. Opponents make the points that stereotactic atlases have been based upon rectilinear approaches to the deep brain targets, placing the guide tube through the ventricle avoids deflection, and blood vessels can be avoided. We prefer minimal angulations (1 to 8 degrees) to allow the most rectilinear approach possible (offset error of 1 mm through Vim) while avoiding the lateral ventricle most of the time. The entry point generally correlates to a ring angle of 60 to 70 degrees relative to the AC–PC line if the approach is applied in a rectilinear fashion to parallel the borders of the Vim.67 An overlay of a Guiot derivation of the thalamic subnuclei location based on the AC–PC line and the height of the thalamus on MRI of a DBS lead illustrates this point (Fig. 11.7). The target coordinates should be considered as only the initial starting point; physiological confirmation is required. Because the initial target point for many surgeons will vary from Vop to Vim, recommended target coordinates may vary from 1 to 7 mm posterior to the midpoint of the AC–PC line. Similarly, the lateral coordinates from the midline vary from 12 to 15 mm and the vertical coordinates vary from 0 to 3 mm above the AC–PC line. We measure 4 mm anterior to the PC along the intercommissural line to identify the border of the Vc. We prefer to use MER and neurological examination intraoperatively to identify the Vc nucleus first, and then move anteriorly to the appropriate position in the Vim (Fig. 11.8). The DBS lead needs to be placed 3 to 4 mm anterior to the Vc hand area. For direct targeting, the lateral distance depends on the observed location of the internal capsule on MRI, which is more accurate than ventriculography.68 The lateral coordinate is selected as 3 mm from the edge of the internal capsule. For indirect targeting, the thalamotomy target is 14 to 16 mm lateral to the midline or 11.5 mm plus half the width of the third ventricle from midline and depth is at the level of the AC-PC plane. For DBS, the target (Vim/Vop border) is 11 to 14 mm or 10 mm plus half the width of the third ventricle from midline because the thalamic-capsular border moves medially. For predominantly head and neck tremor a more medial approach is used. Because of the inherent variability in biological systems, radiographic determination of the target may be inaccurate, varying as much as several millimeters from physiologically determined sites. By combining MER and macroelectrode stimulation techniques with conventional radiographic methods, we believe accurate localization of the optimal target site can be greatly improved. Precise localization allows restriction of the size of the electrical field (lower voltage and longer battery life) while maintaining its effectiveness and minimizing potential complications. If electrophysiological recordings are initiated greater than 30 mm above target, identification of the caudate nucleus may be useful in plotting the tract on an atlas. Passage through the caudate nucleus will yield insertional activity (action potentials stimulated by MER movement that rapidly abates at rest) that would not be identified if the tract were too posterior or very lateral or if the nucleus were markedly atrophic.
Stereotactic Frame Placement
Anatomical Targeting
Surgical Exposure and Trajectory
Physiological Targeting
Deep Brain Stimulation Lead Placement and Anchoring
Internal Pulse Generator Placement
Deep Brain Stimulation Programming
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Neupsy Key
Fastest Neuropsychology Insight Engine

