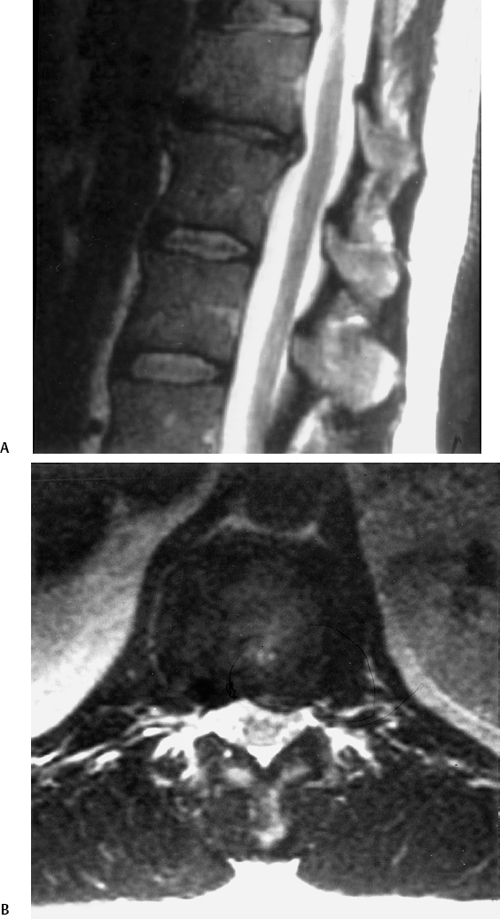
12 I. General considerations A. Thoracic pain may be due to several different etiologies (Table 12–1). 1. Incidence is ~15%. 2. Frequently presents in the fourth to sixth decade of life 3. Clinical presentation a. May be either radicular or myelopathic (1) Thoracic canal is relatively small. (2) Subtle myelopathic symptoms are significant. (3) Radiculopathy involves radiating pain around the associated rib. B. Diagnosis 1. Thoracic disk herniation is frequently seen on magnetic resonance imaging (MRI). a. MRI is most useful because of the wide field of view. (1) Provides information regarding the status of disk degeneration and spinal canal impingement (Fig. 12–1) (2) High false-positive rate (3) Also useful in ruling out infections and tumors b. Myelogram/computed tomography (CT) scan (1) More accurate assessment of spinal cord impingement (Fig. 12–2) 2. Thoracic stenosis a. Ossification of posterior longitudinal ligament (1) Common in Asian populations b. Ossification of ligamentum flavum (1) Posterior spinal cord compression (2) Treated with posterior thoracic decompression c. Spondylosis
Degenerative Thoracic Spine Conditions
| Category | Etiologies |
| Cardiovascular |
|
| Pulmonary |
|
| Mediastinal |
|
| Intra-abdominal |
|
| Gastrointestinal |
|
| Retroperitoneal |
|
| Neurological |
|
| Infectious |
|
| Traumatic |
|
| Neoplastic |
|
| Metabolic |
|
| Miscellaneous |
|
II. Treatment of thoracic disk disease
A. Conservative modalities
1. Nonsteroidal antiinflammatory drugs
2. Exercise program