Diagnostic tests are performed to detect such brain diseases or disorders as congenital defects and anomalies, perinatal defects, ventricular abnormalities, epilepsies, degenerative diseases, and space-occupying lesions. This last category includes neoplasms, infections, and vascular lesions such as arteriovenous malformations. (See Neuropsychological testing.)
Infectious diseases may also be diagnosed, including those caused by bacteria, such as meningitis; viruses, such as encephalitis or polioencephalomyelitis; spirochetes, such as neurosyphilis; parasitic infestations, such as toxoplasmosis (common in patients with acquired immunodeficiency syndromes); and fungal and related infections. Demyelinating diseases, such as multiple sclerosis; cerebrovascular disorders, including stroke, transient ischemic attacks, aneurysms of the blood vessels, and subdural and subarachnoid hemorrhages; and disorders of the skull, vertebral column, and other nonneural tissues may also be diagnosed using the tests presented in this chapter.
These tests may also detect such disorders of the brain stem and cranial nerves as vascular insufficiency due to obstruction to specific regions of the brain stem, cranial nerve syndromes (such as trigeminal neuralgia), headache disorders, and congenital disorders that occur as distortions of normal relationships between the skull and vertebral column or as abnormal formations of the skull base.
NEUROPSYCHOLOGICAL TESTING
Rather than documenting physiologic changes in the nervous system, neuropsychological testing evaluates the effects of neurologic disorders on a patient’s ability to function.
Indications
Neuropsychological tests can evaluate cognitive functioning, including general intelligence, attention span, memory, and judgment as well as motor, sensory, and speech ability. Certain tests can assess emotional lability, quality of language production, abstraction, distractibility, persistence, or the ability to sequence learned activities. The neuropsychologist chooses the appropriate test based on the reason for the assessment and the skills being assessed.
Besides determining the type and extent of functional deficits in the patient with a known neurologic illness, neuropsychological tests can diagnose organic brain dysfunction and dementia. They’re also used to determine whether an injured patient can return to a previous occupation or should be declared disabled. What’s more, these tests can assess the extent of rehabilitation or vocational training required before the patient can fully function again. Neuropsychological tests may be performed before and after a major neurosurgical or radiologic procedure to obtain baseline information for comparison with postprocedural information. A neuropsychologist administers the series of paper-and-pencil tests, possibly in combination with other tests using puzzles, blocks, or word or recall games. The neuro-psychologist explains each test to the patient before administration.
Precautions
Because these tests are mentally demanding and lengthy, they may tire the patient. If possible, withdraw medications that affect his ability to concentrate before the test. The patient should be well rested and free from sedatives, if possible, before testing. Any physiologic problem that may interfere with mental function or level of consciousness, such as fever or electrolyte imbalance, should be treated before testing to ensure that results are as accurate as possible.
The spinal cord may be affected by metastasis from noncentral nervous system primary tumors that spread to the vertebrae and meninges, producing extradural tumors that distort the spinal cord or interrupt cerebrospinal fluid (CSF) flow in the spinal subarachnoid spaces. This, in turn, causes a block in CSF circulation accompanied by spinal cord dysfunction. In addition to the spinal cord, the brain stem may also be affected by Guillain-Barré syndrome, which is typically a myeloradiculopathy.
Because disorders of the peripheral nervous system are in many cases toxic or metabolic in origin, the tests covered in this chapter are generally not as useful for investigating exposure to toxins or as a systemic metabolic workup. In addition, the diagnosis of peripheral neuropathies commonly depends on nerve biopsy, which allows the identification of specific pathologic change in the nerve fibers. Similarly, when attempting to identify myopathies or muscle disorders, muscle biopsy is commonly the preferred diagnostic tool.
The patient’s ability to function with neurologic disorders can be evaluated by other tests.
LABORATORY TESTS
BACTERIAL MENINGITIS ANTIGEN
The bacterial meningitis antigen test can detect specific antigens of Streptococcus pneumoniae, Neisseria meningitidis, Haemophilus influenzae type B, or group B streptococci, the principal etiologic agents in meningitis. Although cerebrospinal fluid (CSF) and urine are the preferred sample for analysis, the test may also be performed using samples of serum, pleural fluid, and joint fluid. Positive results identify the specific bacterial antigen: S. pneumoniae, N. meningitidis, H. influenzae type B, or group B streptococci.
Nursing considerations
Explain the purpose of the test to the patient and his family, as appropriate.
Inform the patient that this test requires a specimen of urine or CSF. Explain who will perform the procedure and when.
If a CSF specimen is required, describe how it will be obtained by a lumbar puncture procedure.
Explain to the patient that he may experience discomfort from the needle puncture.
Advise the patient that headache is the most common complication of lumbar puncture, but that his cooperation during the test minimizes such an effect.
Verify that the patient or a family member has signed an informed consent form for the lumbar puncture.
Collect a 10-ml urine specimen or a 1-ml CSF specimen in a sterile container.
Maintain specimen sterility during collection.
Wear gloves when obtaining or handling the specimen.
Make sure the cap is tightly fastened on the specimen container.
Place the specimen on a refrigerated coolant, and send it to the laboratory immediately.
CEREBROSPINAL FLUID ANALYSIS
Cerebrospinal fluid (CSF), a clear substance that circulates in the subarachnoid space, has many vital functions. It protects the brain and spinal cord from injury and transports products of neurosecretion, cellular biosynthesis, and cellular metabolism through the central nervous system (CNS).
For qualitative analysis, CSF is most commonly obtained by lumbar puncture (usually between the third and fourth lumbar vertebrae) and, rarely, by cisternal or ventricular puncture. A CSF specimen may also be obtained during other neurologic tests, such as myelography or from a ventriculostomy tube. CSF analysis aids the diagnosis of viral or bacterial meningitis, subarachnoid or intracranial hemorrhage, tumors, brain abscesses, neurosyphilis, and chronic CNS infections. (See Findings in cerebrospinal fluid analysis, pages 106 and 107.)
Normally, the CSF pressure is recorded and the appearance of the specimen is checked. Three tubes are collected routinely and are sent to the laboratory for protein, sugar, and cell analysis as well as for serologic testing, such as the Venereal Disease Research Laboratory test for neurosyphilis. A separate specimen is also sent to the laboratory for culture and sensitivity testing. Electrolyte analysis and Gram stain may be ordered as supplementary tests. CSF electrolyte levels are of special interest in the patient with abnormal serum electrolyte levels or CSF infection and in the patient receiving hyperosmolar agents.
FINDINGS IN CEREBROSPINAL FLUID ANALYSIS
TEST
NORMAL
ABNORMALITY
IMPLICATIONS
Pressure
50 to 180 mm H2O
Increase
Increased intracranial pressure
Decrease
Spinal subarachnoid obstruction above puncture site
Appearance
Clear, colorless
Cloudy
Infection
Xanthochromic or bloody
Subarachnoid, intracerebral, or intraventricular hemorrhage; spinal cord obstruction; traumatic tap (usually noted only in initial specimen)
Brown, orange, or yellow
Elevated protein levels, red blood cell (RBC) breakdown (blood present for at least 3 days)
Systemic hypoglycemia, bacterial or fungal infection, meningitis, mumps, postsubarachnoid hemorrhage
Cell count
0 to 5 white blood cells
Increase
Active disease: meningitis, acute infection, onset of chronic illness, tumor, abscess, infarction, demyelinating disease
No RBCs
RBCs
Hemorrhage or traumatic lumbar puncture
Venereal Disease Research Laboratories test for syphilis and other serologic tests
Nonreactive
Positive
Neurosyphilis
Chloride
118 to 130 mEq/L (SI, 118 to 130 mmol/L)
Decrease
Infected meninges
Gram stain
No organisms
Gram-positive or gram-negative organisms
Bacterial meningitis
Nursing considerations
Describe the procedure to the patient and explain that CSF analysis analyzes the fluid around the spinal cord.
Inform the patient that he need not restrict food and fluids.
Tell the patient who will perform the procedure and where and when it will take place.
Advise the patient that headache is the most common complication of lumbar puncture, but reassure him that his cooperation during the test helps minimize such an effect.
If the specimen will be obtained by an invasive procedure, verify that the patient or a family member has signed an informed consent form for the proceudre. A consent form isn’t necessary if the specimen is obtained from an existing ventriculostomy.
If the patient is unusually anxious, assess and report his vital signs.
If CSF pressure is elevated, assess the patient’s neurologic status every 15 minutes for 4 hours. If he’s stable, assess him every hour for 2 hours and then every 4 hours or according to the pretest schedule.
During the procedure, closely observe the patient for adverse reactions, such as elevated pulse rate, pallor, or clammy skin. Report any significant changes immediately.
Record the collection time on the test request form. Send the form and labeled specimens to the laboratory immediately after collection.
RED FLAG
Watch the patient for complications of lumbar puncture, such as reaction to the anesthetic, meningitis, bleeding into the spinal canal, and cerebellar tonsillar herniation and medullary compression. Signs of meningitis include fever, neck rigidity, and irritability; signs of herniation include decreased level of consciousness, changes in pupil size and equality, altered vital signs (including widened pulse pressure, decreased pulse rate, and irregular respirations), and respiratory failure.
SERUM ANTIDIURETIC HORMONE
Antidiuretic hormone (ADH), also called vasopressin, promotes water reabsorption in response to increased osmolality (water deficiency with high concentration of sodium and other solutes). In response to decreased osmolality (water excess), reduced secretion of ADH allows increased excretion of water to maintain fluid balance. Along with aldosterone, ADH helps regulate sodium, potassium, and fluid balance. It also stimulates vascular smooth-muscle contraction, causing an increase in arterial blood pressure.
This relatively rare test may be ordered as part of dehydration or hypertonic saline infusion testing, which determines the body’s response to states of hyperosmolality. It may also identify pituitary diabetes insipidus, nephrogenic diabetes insipidus (congenital or familial), and syndrome of inappropriate antidiuretic hormone (SIADH).
ADH values range from 1 to 5 pg/ml (SI, 1 to 5 mg/L). For example, if serum osmolality is less than 285 mOsm/kg, ADH is normally less than 2 pg/ml (SI, < 2 mg/L); if it’s greater than 290 mOsm/kg, ADH may range from 2 to 12 pg/ml (SI, 2 to 12 mg/L). Absent or below-normal ADH levels indicate pituitary diabetes insipidus, resulting from a neurohypophyseal or hypothalamic tumor, viral infection, metastatic disease, sarcoidosis, tuberculosis, Hand-Schüller-Christian disease, syphilis, neurosurgical procedures, or head trauma.
Normal ADH levels in the presence of signs of diabetes insipidus (such as polydipsia, polyuria, and hypotonic urine) may indicate the nephrogenic form of the disease, marked by renal tubular resistance to ADH; however, levels may rise if the pituitary gland tries to compensate.
Elevated ADH levels may also indicate SIADH, possibly as a result of bronchogenic carcinoma, acute porphyria, hypothyroidism, Addison’s disease, cirrhosis of the liver, infectious hepatitis, severe hemorrhage, or circulatory shock.
Nursing considerations
Explain to the patient that the test is going to measure his hormonal secretion levels and may aid in pinpointing the cause of his symptoms.
Instruct the patient to fast and limit physical activity for 10 to 12 hours before the test.
Tell the patient that the test requires a blood sample. Explain who will perform the venipuncture and when.
Explain to the patient that he may experience slight discomfort from the tourniquet and the needle puncture.
Withhold medications that may cause SIADH before the test, as ordered. If they must be continued, note this on the laboratory request.
Make sure the patient is relaxed and recumbent for 30 minutes before the test.
Perform a venipuncture and collect the sample in a plastic collection tube (without additives) or a chilled EDTA tube. Make sure you use a syringe and collection tube made of plastic because the fragile ADH degrades on contact with glass.
Immediately send the sample to the laboratory, where serum must be separated from the clot within 10 minutes.
Perform a serum osmolality test at the same time to help interpret the results.
Apply direct pressure to the venipuncture site until bleeding stops.
If a hematoma develops at the venipuncture site, apply warm soaks.
Instruct the patient that he may resume his usual diet, activities, and medications discontinued before the test, as ordered.
NONINVASIVE TESTS OR PROCEDURES
COMPUTED TOMOGRAPHY SCAN, INTRACRANIAL
An intracranial computed tomography (CT) scan records a series of tomograms, which are translated by a computer and displayed on a monitor, representing cross-sectional images of various layers of the brain. This technique can reconstruct cross-sectional, horizontal, sagittal, and coronal plane images. Hundreds of thousands of readings of radiation levels absorbed by brain tissues may be combined to depict anatomic slices of varying thickness. Specificity and accuracy are enhanced by the degree of resolution, which depends on the number of radiation density calculations made by the computer, and through the use of contrast medium. Although magnetic resonance imaging (MRI) has surpassed CT scanning in diagnosing neurologic anatomy and pathology, the CT scan is more widely available and cost-effective and can be performed more easily in acute situations.
In addition to accurately diagnosing intracranial lesions and bleeding, CT scans may also be used to monitor the effects of surgery, radiation therapy, chemotherapy on intracranial tumors, or to serve as a guide for cranial surgery.
The tissue density (water content) depends on the amount of radiation that has passed through it. For example, normal tissue densities appear as white, black, or shades of gray on the computed image. Bone, the densest tissue, appears white; ventricular and subarachnoid cerebrospinal fluid, the least dense, appears black. Brain matter appears in shades of gray.
In addition to examining density, structures are also evaluated according to their size, shape, and position. Areas of altered density (may appear lighter or darker) or displaced vasculature or other structures may indicate an intracranial tumor, a hematoma, cerebral atrophy, an infarction, edema, or congenital anomalies such as hydrocephalus.
Intracranial tumors vary significantly in appearance and characteristics. Metastatic tumors generally cause extensive edema in early stages and can usually be defined by contrast enhancement. Primary tumors vary in density and in their capacity to cause edema, displace ventricles, and absorb the contrast medium in contrast enhancement. Astrocytomas, for example, usually have low densities; meningiomas have higher densities and can generally be defined with contrast enhancement; glioblastomas, usually ill defined, are also enhanced after injection of a contrast medium.
Because the high density of blood contrasts markedly with low-density brain tissue, it’s normally easy to detect subdural and epidural hematomas and other acute hemorrhages with contrast enhancement.
Cerebral atrophy customarily appears as enlarged ventricles with large sulci. Cerebral infarction may appear as low-density areas at the obstruction site or may not be apparent, especially within the first 24 hours or if the infarction is small or doesn’t cause edema. With contrast enhancement, the infarcted area may not show in the acute phase, but will show clearly after resolution of the lesion. Cerebral edema usually appears as an area of marked generalized decreased density. In children, enlargement of the fourth ventricle generally indicates hydrocephalus.
Normally, the cerebral vessels don’t appear on CT images. However, in the patient with arteriovenous malformation, cerebral vessels may appear with slightly increased density. Contrast enhancement allows a better view of the abnormal area, but MRI is now the preferred procedure for imaging cerebral vessels. Another technology for obtaining brain images is positron emission tomography. (See Understanding PET and SPECT.)
UNDERSTANDING PET AND SPECT
Like computed tomography (CT) scanning and magnetic resonance imaging, positron emission tomography (PET) and single-photon emission computed tomography (SPECT) provide brain images through sophisticated computer reconstruction algorithms. However, PET and SPECT images detail brain function as well as structure and thus differ significantly from the images provided by these other advanced techniques. PET and SPECT combine elements of CT scanning and conventional radionuclide imaging. For example, they measure the emissions of injected radioisotopes and convert them to a tomographic image of the brain. PET scanning uses radioisotopes of biologically important elements—oxygen, nitrogen, carbon, and fluorine—that emit particles called positrons; whereas SPECT scanning uses gamma radiation with radionuclides within the brain.
How it works
During PET and SPECT, pairs of gamma rays are emitted; the scanner detects them and relays the information to a computer for reconstruction as an image. PET scanners omit positrons that can be chemically “tagged” to biologically active molecules, such as carbon monoxide, neurotransmitters, hormones, and metabolites (especially glucose), enabling study of their uptake and distribution in brain tissue. For example, blood tagged with 11 Ccarbon monoxide allows study of hemodynamic patterns in brain tissue; tagged neurotransmitters, hormones, and drugs allow mapping of receptor distribution. SPECT scanners use radionucleotides labeled with iodine or hexamethylpropylene amine oxime to detect blood flow.
Isotope-tagged glucose (which penetrates the blood-brain barrier rapidly) allows dynamic study of brain function because PET scans can pinpoint the sites of glucose metabolism in the brain under various conditions. Researchers expect PET and SPECT scanning to prove useful in the diagnosis of psychiatric disorders, transient ischemic attacks, amyotrophic lateral sclerosis, Parkinson’s disease, Wilson’s disease, multiple sclerosis, seizure disorders, cerebrovascular disease, and Alzheimer’s disease. The rationale behind this theory is that all of these disorders may alter the location and patterns of cerebral glucose metabolism.
Cost factors
PET scanning is a costly test because the radioisotopes used have very short half-lives and must be produced at an on-site cyclotron and attached quickly to the desired tracer molecules.
Nursing considerations
Tell the patient that a series of images will be taken of his brain. Describe who will perform the test and where it will take place. Explain that the test will cause minimal discomfort.
Explain to the patient that intracranial CT permits assessment of the brain.
Make sure that any paperwork required by the facility concerning CT scans is complete.
Unless contrast enhancement is scheduled, inform the patient that there are no food or fluid restrictions. If contrast enhancement is scheduled, instruct him to fast for 4 hours before the test.
Tell the patient that he’ll be positioned on a moving CT bed with his head immobilized and his face uncovered. The head of the table will then be moved into the scanner, which rotates around his head and makes a swirling sound.
If a contrast medium is used, tell the patient that he may feel flushed and warm and may experience a transient headache, a salty or metallic taste, or nausea and vomiting after the contrast medium is injected. Reassure him that these reactions are normal.
Instruct the patient to wear a gown (outpatients may wear comfortable clothing) and to remove all metal objects from the CT scan field.
If the patient is restless or apprehensive, a sedative may be prescribed.
If a contrast medium will be used, check the patient’s history for hypersensitivity to shellfish, iodine, or contrast media, and mark your findings in his chart. Inform the physician of any sensitivities because he may order prophylactic medications or may choose not to use contrast enhancement.
After administration of a contrast medium, watch the patient for residual adverse reactions (headache, nausea, and vomiting) and inform him that he may resume his usual diet.
COMPUTED TOMOGRAPHY SCAN, SPINAL
Much more versatile than conventional radiography, a spinal computed tomography (CT) scan records detailed high-resolution images in the cross-sectional, longitudinal, sagittal, and lateral planes. Multiple X-ray beams from a computerized body scanner are directed at the spine from different angles; these pass through the body and strike radiation detectors, producing electrical impulses. A computer then converts these impulses into digital information, which is displayed as a three-dimensional image on a monitor. Storage of the digital information allows electronic recreation and manipulation of the image, creating a permanent record of the images to enable reexamination without repeating the procedure.
CT scans are helpful in defining the lesions causing spinal cord compression. Metastatic disease and discogenic disease with osteophyte formation and calcification are examples of pathologic processes diagnosed by CT scans. Since the advent of magnetic resonance imaging, CT scans are used less frequently to diagnose infection, abscesses, hematomas, and some disk herniations. However, they continue to be useful in monitoring the effects of spinal surgery or therapy.
In the spinal CT image, normal tissue appears white, black, or gray, depending on its density. Vertebrae, the densest tissues, are white; cerebrospinal fluid is black; and soft tissues appear in shades of gray.
By highlighting areas of altered density and depicting structural malformation, CT scanning can reveal all types of spinal lesions and abnormalities. It’s particularly useful in detecting and localizing tumors, which appear as masses varying in density. Measuring this density and noting the configuration and location relative to the spinal cord can usually identify the type of tumor. For example, a neurinoma (schwannoma) appears as a spherical mass dorsal to the cord. A darker, wider mass lying more laterally or ventrally to the cord may be a meningioma.
CT scans also reveal degenerative processes and structural changes in detail. Herniated nucleus pulposus shows as an obvious herniation of disk material with unilateral or bilateral nerve root compression; if the herniation is midline, spinal cord compression is evident. Cervical spondylosis shows as cervical cord compression due to bony hypertrophy of the cervical spine; lumbar stenosis, as hypertrophy of the lumbar vertebrae, causing cord compression by decreasing space within the spinal column. Facet disorders show as soft-tissue changes, bony overgrowth, and spurring of the vertebrae, which result in nerve root compression. Fluid-filled arachnoidal and other paraspinal cysts show as dark masses displacing the spinal cord. Vascular malformations, evident after contrast enhancement, show as masses or clusters, usually on the dorsal aspect of the spinal cord.
Congenital spinal malformations, such as meningocele, myelocele, and spina bifida, show as abnormally large, dark gaps between the white vertebrae.
Nursing considerations
Tell the patient that a series of scans will be taken of his spine. Explain who will perform the procedure and where it will take place.
Explain that spinal CT allows visualization of his spine.
Make sure that any paperwork required by the facility concerning CT scans is complete.
If contrast medium isn’t ordered, tell the patient that he need not restrict food and fluids. If contrast medium is ordered, instruct him to fast for 4 hours before the test.
Reassure the patient that the procedure is painless, but that he may find having to remain still for a prolonged period uncomfortable.
For the patient with significant back pain, administer prescribed analgesics before the scan.
Explain to the patient that he’ll be positioned on an X-ray table inside a CT body scanning unit and he’ll be told to lie still because movement during the procedure may cause distorted images. The computer-controlled scanner will revolve around him, taking multiple scans.
If a contrast medium is used, tell the patient that he may feel flushed and warm and may experience a transient headache, a salty or metallic taste, and nausea or vomiting after injection of the contrast medium. Reassure him that these reactions are normal.
Instruct the patient to wear a radiologic examining gown and to remove all metal objects and jewelry.
Check the patient’s history for hypersensitivity reactions to iodine, shellfish, or contrast media. If such reactions have occurred, note them in the patient’s chart and notify the physician, who may order prophylactic medications or choose not to use contrast enhancement.
If the patient appears restless or apprehensive about the procedure, a mild sedative may be prescribed.
If a contrast medium was used, watch the patient for residual adverse reactions (headache, nausea, and vomiting) and inform him that he may resume his usual diet.
RED FLAG
Observe the patient for signs and symptoms of a hypersensitivity reaction, including pruritus, rash, and respiratory difficulty, for 30 minutes after the contrast medium has been injected.
ELECTROENCEPHALOGRAM
An EEG records the brain’s electrical activity through electrodes attached to the patient’s scalp. This information is then transmitted to an electroencephalograph, which records the resulting brain waves on recording paper. The procedure may be performed in a special laboratory or by a portable unit at the bedside. Ambulatory recording EEGs are available for the patient to wear at home or at the workplace to record the patient as he performs his normal daily activities. Continuous-video EEG recording is available on an inpatient basis for identifying epileptic discharges during clinical events or for localization of a seizure focus during surgical evaluation of epilepsy. An EEG can help determine the presence and type of seizure disorder; aid in the diagnosis of intracranial lesions, such as abscesses and tumors; evaluate the brain’s electrical activity in metabolic disease, cerebral ischemia, head injury, meningitis, encephalitis, mental retardation, psychological disorders, and effects of certain drugs; and evaluate altered states of consciousness or brain death
EEG records a portion of the brain’s electrical activity as waves; some are irregular, whereas others demonstrate frequent patterns. Among the basic waveforms are the alpha, beta, theta, and delta rhythms.
Alpha waves occur at a frequency of 8 to 11 cycles/second in a regular rhythm. They’re present only in the waking state when the patient’s eyes are closed; usually, they disappear with visual activity or mental concentration. Beta waves occur at a frequency of 13 to 30 cycles/second. They’re generally associated with anxiety, depression, and use of sedatives and are seen most readily in the frontal and central regions of the brain. Theta waves occur at a frequency of 4 to 7 cycles/second. They’re most common in children and young adults and appear in the frontal and temporal regions. Delta waves occur at a frequency of 0.5 to 3.5 cycles/second. They normally occur only in young children and during sleep. (See Comparing EEG tracings.)
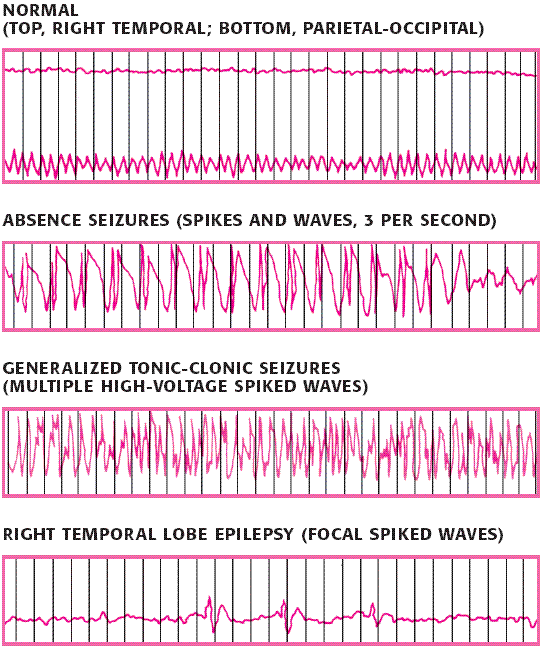
In the patient with epilepsy, EEG patterns may identify the specific disorder. In absence seizures, the EEG shows spikes and waves at a frequency of 3 cycles/second. In generalized tonicclonic seizures, it generally shows multiple, high-voltage, spiked waves in both hemispheres. In temporal lobe epilepsy, the EEG usually shows spiked waves in the affected temporal region. In the patient with focal seizures, it usually shows localized, spiked discharges.
COMPARING EEG TRACINGS
The following tracings are examples of regular and irregular brain electrical activity as recorded by an EEG.
In the patient with an intracranial lesion, such as a tumor or abscess, the EEG may show slow waves (usually delta waves but possibly unilateral beta waves). Vascular lesions, such as cerebral infarcts and intracranial hemorrhages, generally produce focal abnormalities in the injured area.
Generally, any condition that causes a diminishing level of consciousness alters the EEG pattern in proportion to the degree of consciousness lost. For example, in a patient with a metabolic disorder, an inflammatory process (such as meningitis or encephalitis), or increased intracranial pressure, the EEG shows generalized, diffuse, and slow brain waves.
The most pathologic finding of all is an absent EEG pattern—a “flat” tracing (except for artifacts), which may indicate brain death.
Nursing considerations
Explain to the patient that an EEG records the brain’s electrical activity.
Describe the procedure to the patient and family members and answer all questions.
Explain that he must withhold caffeine before the test; other than this, there are no food or fluid restrictions. However, tell him that skipping the meal before the test can cause relative hypoglycemia and alter the brain wave pattern.
Only gold members can continue reading. Log In or Register to continue