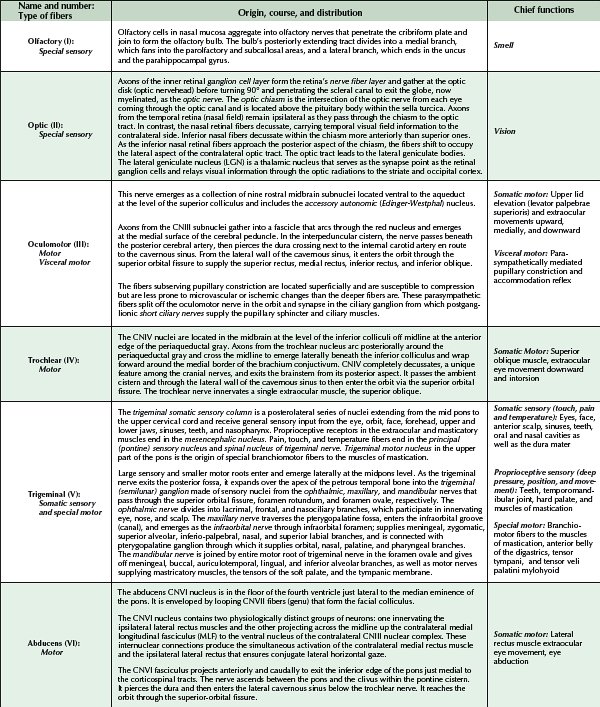
Cranial nerve motor nuclei are located medially, whereas the sensory nuclei are found generally more lateral. Three types of motor nuclei are present innervating voluntary striated muscles (somatic), muscles of facial expressions and mastication (special motor derived from embryonic branchial arch structures), and autonomic smooth muscles (visceral). Each cranial nerve serves a regional skull area and may provide more than one function to that area and therefore is not restricted to a single nucleus or nerve type. For example, the facial nerve provides voluntary motor innervations to the face as well as taste special sensation to the anterior tongue. The pure motor nerves (except for perhaps some proprioceptive function) are the oculomotor III, trochlear IV, abducens VI, spinal accessory nerve XI, and hypoglossal XI. The special sensory nerves are the olfactory, optic, and vestibulocochlear. Mixed cranial nerves are the trigeminal V, facial VII, glossopharyngeal IX, and vagus X. A summary of the origin, course, and distribution of each cranial nerve is outlined on the next plates.
Cranial neuropathies may manifest as a single cranial neuropathy or, less commonly, as multiple cranial neuropathies. Single cranial neuropathies are discussed in their respective sections. For example, Bell palsy is reviewed in the cranial nerve VII (facial nerve) section. Multiple cranial neuropathies involve any combination of cranial nerves, although cranial nerves III, V, VI, and VII are the most commonly affected in most clinical series. The manifestations of multiple cranial neuropathies reflect the sites of injury and function of the cranial nerves affected. The many different causes of multiple cranial neuropathies include infectious, neoplastic, autoimmune disease, trauma, and vascular disease. Infections associated with multiple cranial neuropathies include Lyme disease, tuberculous meningitis, cryptococcus, histoplasmosis, botulism, mucormycosis, certain viruses (e.g., herpes simplex virus, varicella-zoster virus) and bacterial meningitis. Guillain-Barré syndrome (GBS) and the Miller Fisher variant of GBS are monophasic, autoimmune polyradiculoneuropathies that can frequently involve multiple cranial nerves. Neoplasms cause multiple cranial neuropathies either by direct compression and local extension, such as with meningiomas, schwannomas, and nasopharyngeal tumors, or by diffuse dissemination and meningeal infiltration, such as with lymphoma and various carcinomas. Myasthenia gravis (MG) mimics multiple cranial neuropathies but the site of autoimmune attack in MG is directed against the postsynaptic muscle end rather than the nerve.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


