Chapter 17 Does Early Treatment Influence the Long-Term Outcome of Epilepsy?
Seizure Recurrence following a First Seizure
Studies assessing the prognosis for patients presenting with their first seizure or seizures have tended to focus on seizure recurrence rates. For patients presenting with a single seizure, many observational studies, both prospective and retrospective, have assessed seizure recurrence rates, many of which have been summarized in a systematic review and meta-analysis reported by Berg and Shinnar.1 Thirteen first seizures studies were included in this systematic review, and the overall seizure recurrence risk was 46% (44 to 49) and for the subset of 5 prospective studies was 40% (37 to 43). The 2-year recurrence risk was 42% (39 to 44) across all studies and 36% (32 to 39) for the subset of prospective studies. There was a significantly higher recurrence risk for patients with partial onset seizures, an abnormal EEG, and neurological abnormality (learning difficulty, neurological signs, etc.). Thus, for the majority of patients presenting with a single seizure, the risk of a recurrence is low, and given the potential side effects of antiepileptic drugs, antiepileptic drug treatment has not been routinely recommended.
The most reliable method to assess the influence of antiepileptic drug treatment on recurrence rates and other outcomes is the randomized controlled trial. Such a study would randomly allocate patients to treatment or no treatment (or immediate or deferred treatment) and ideally should be large enough to allow subgroup analyses, most commonly in regression analyses, allowing the identification of patient characteristics that influence seizure recurrence risks and the magnitude of any treatment effect. To date, five published randomized controlled trials have examined the impact of antiepileptic drug treatment following a first seizure,2–6 and the key characteristics of these trials are summarized in Table 17-1.
TABLE 17–1 Randomized Controlled Trials Comparing Antiepileptic Drug Treatment Versus No Treatment Following a First Seizure
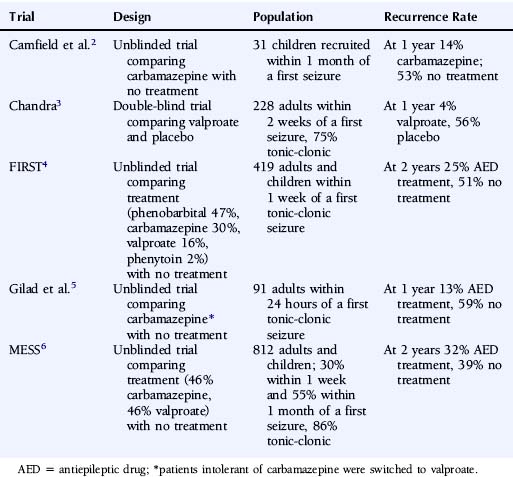
These trials consistently show a lower seizure recurrence rate with antiepileptic drug treatment compared to no treatment or placebo. There are, however, substantial differences among these trials in the estimated recurrence risks, with the 1- to 2-year recurrence risk ranging from 4 to 32% for AED-treated patients and 39 to 59% for untreated patients. These differences are most likely explained by differences in study design and patient populations in terms of factors such as time between seizure and randomization, seizure type, and age. Only two trials recruited sufficient patients to examine patient predictors of outcome. In the FIRST trial4,7 age <16 years, secondarily generalized seizures, remote symptomatic seizures, and epileptiform changes on the EEG were associated with a higher risk of recurrence, whereas acute treatment with benzodiazepines was associated with a lower risk of recurrence.
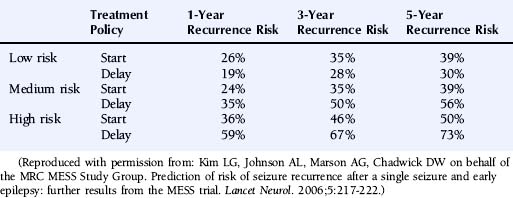
The multicenter study of early epilepsy and single seizures (MESS trial)6 recruited 812 patients following a single seizure and 631 following two or more seizures. Regression modeling showed that the number of seizures before randomization, an abnormal EEG, and the presence of a neurological abnormality (learning disability or neurological signs) increased the risk of a seizure recurrence.8 This allowed the creation of a prognosis index to stratify patients in the groups with a low, medium, or high risk of seizure recurrence as summarized in Table 17-2. The recurrence risks estimated for these groups are given in Table 17-3.
TABLE 17–2 Prognostic Index from the MESS Trial
| Prognostic Index | |
|---|---|
| Starting Value | |
| Single seizure | 0 |
| Two or three seizures | 1 |
| Four or more seizures | 2 |
| Add if Present | |
| Neurological disorder of deficit | 1 |
| Abnormal EEG | 1 |
| Risk Classification Group | Final Score |
| Low risk | 0 |
| Medium risk | 1 |
| High risk | 2–4 |
Reproduced with permission from: Kim LG, Johnson AL, Marson AG, Chadwick DW on behalf of the MRC MESS Study Group. Prediction of risk of seizure recurrence after a single seizure and early epilepsy: further results from the MESS trial. Lancet Neurol. 2006;5:217-222.
Seizure Recurrence following a Second Seizure
The risk of unprovoked seizures following a second seizure has not been examined in a prospective population-based study of patients untreated with antiepileptic drugs. Antiepileptic drugs became accepted practice for patients with epilepsy before robust epidemiological methods had been applied to examine the natural history of untreated epilepsy. It would now, of course, be considered unethical to deny a population of patients a treatment that is believed to be effective in order to examine this. The risk of seizure recurrence following two unprovoked seizures has been examined by Hauser et al.,9 who prospectively followed up 204 patients, 87% of whom were on antiepileptic drug treatment following their second seizure. The risk of a third seizure following a second was 32% (21 to 43) at 3 months, 41% (29 to 53) at 6 months, 57% (45 to 70) at 12 months, and 73% (59 to 87) at 4 years. The risk of a third seizure was higher in patients with remote symptomatic seizures than those with idiopathic or cryptogenic seizures, hazard ratio 1.9 (1.0 to 3.4). Other factors such as seizure type, EEG abnormality, or neurological abnormality were not significantly associated with a third seizure. The risk of a fourth seizure following a third was 31% (16 to 46) at 3 months, 48% (32 to 64) at 6 months, 61% (44 to 77) at 1 year and 76% (60 to 90) at 3 years. Shinnar et al. found similar results in a cohort of 407 children prospectively followed after their first seizure.10
Thus, in contrast to patients with a first seizure, the risk of an additional seizure following a second or third unprovoked seizure is high, even with the use of antiepileptic drugs. Given this finding in their paper, Hauser and colleagues recommend that patients with two or more unprovoked seizures should start antiepileptic drug treatment, although this study, by design, is unable to define the magnitude of any effect that antiepileptic drug treatment might have on seizure recurrence rates. To address this question, we need data from randomized controlled trials comparing treatment with no treatment for a cohort of patients with newly diagnosed epilepsy. No such trial has ever been undertaken and would now be considered unethical and would certainly contravene the Declaration of Helsinki.11 At present, therefore, for patients with newly diagnosed epilepsy, we have no robust data that defines the magnitude of any treatment effect of antiepileptic drugs, both for the short-term outcomes (seizure recurrence) discussed earlier, as well as for the longer-term outcomes that are discussed later in this chapter. Despite this, consensus seems to hold that the majority of patients should be offered treatment following two or more seizures, particularly if they have occurred over a relatively short period of time (6 to 12 months). There has continued to be uncertainty regarding the appropriate recommendation for patients with seizures of minor symptomatology (e.g., simple partial seizures), and patients with long periods of time between seizures. Such patients (631) were entered into the MESS study6 when both clinician and patient were uncertain about the need for antiepileptic drug treatment.
Longer-Term Outcomes
Given that up to 30% of patients with epilepsy are drug refractory12 and experience continued seizures and a diminished quality of life, any intervention proven to improve the natural history, by reducing the severity of epilepsy and improving the probability of a long-term remission from seizures, could have important consequences for a large number of patients.13,14 Thus it is important to understand whether the early use of antiepileptic drugs might influence the natural history of epilepsy.
Some have suggested that epilepsy might be a self-facilitating process in which seizures beget seizures,15,16 whereby each seizure causes further neuronal damage and reorganization that increases the probability of the next seizure. This idea was suggested by Gower in 1881, when he suggested that “the tendency of the disease is toward self perpetuation; each attack facilitating the occurrence of the next by increasing the instability of nerve elements.”17
Elwes et al.18 recruited a cohort of 183 patients presenting with a new diagnosis of epilepsy and retrospectively assessed the time interval between successive tonic-clonic seizures prior to their clinic visit. They observed that the time interval between successive seizures became progressively shorter, and the authors suggest that this finding supports early epilepsy being an accelerating process. However, this study may be confounded by its retrospective design, selection bias, seizure type, and perhaps seizure clustering and does not provide evidence of seizures begetting seizures.
Other studies have showed that patients with more seizures or a higher seizure frequency prior to starting antiepileptic drug treatment had a lower rate of remission from seizures.19,20 This finding was again interpreted as indicating that seizures predispose to further seizures and used as an argument for early treatment. However, the number of seizures prior to starting treatment is likely to be correlated with seizure type, with patients with complex partial seizures experiencing a greater number of seizures before starting treatment and having a poorer prognosis, as was the case in these studies. Thus although seizure type and the number of seizures prior to starting treatment may be important prognostic factors, these studies do not necessarily provide evidence of seizures begetting seizures.
Two studies have been undertaken in developing countries, one from Kenya21 and one from Ecuador,22 in which people with untreated epilepsy were ascertained by field workers going door to door. These patients were then offered entry into a randomized controlled trial comparing carbamazepine and phenobarbital; 192 entered the trial in Ecuador, and 302 entered the trial in Kenya. Despite having untreated epilepsy, sometimes for many years, in both studies 53% of patients were seizure free from the 6th to the 12th month of follow-up, which is comparable to outcomes in randomized controlled trials in newly diagnosed populations.23,24 This finding would suggest that the failure to treat epilepsy early does not worsen the prognosis of epilepsy once treatment is started.
There is some animal data that suggests that some antiepileptic drugs may exhibit antiepileptogenic properties. Studies in kindled rats suggest that valproate, phenobarbital, diazepam, vigabatrin, topiramate, levetiraceta, and lamotrigine might have antiepileptogenic properties,25 although the appropriateness of the kindling model for assessing antiepileptogenic properties has been criticized.26 Post-status epilepticus models suggest that topiramate and valproate may have antiepileptogenic properties, although results have been conflicting. Although these models may be appropriate to examine potential antiepileptogenic effects and might equate to patients presenting with prolonged status epilepticus, they do not readily equate to the patient presenting with a single seizure or early epilepsy.
Related posts:
 The Life-Threatening Epilepsies of Childhood and Their Treatment
The Life-Threatening Epilepsies of Childhood and Their Treatment
 The Spectrum of Epilepsies Associated with Generalized Spike-and-Wave Patterns
The Spectrum of Epilepsies Associated with Generalized Spike-and-Wave Patterns
 Epilepsies Due to Monogenic Disorders of Metabolism
Epilepsies Due to Monogenic Disorders of Metabolism
 The Surgery of Temporal Lobe Epilepsy I—Historical Development, Patient Selection, and Seizure Outcome
The Surgery of Temporal Lobe Epilepsy I—Historical Development, Patient Selection, and Seizure Outcome
 Mechanisms of Action of Levetiracetam and Newer SV2A Ligands
Mechanisms of Action of Levetiracetam and Newer SV2A Ligands
 Cortical Myoclonus and Epilepsy: Overlap and Differences
Cortical Myoclonus and Epilepsy: Overlap and Differences



