Bipolar disorder is a serious mental disorder in which recurrences of mania, hypomania, and depression are the rule, and in perhaps one third of the patients symptoms become chronic. Bipolar disorder’s seriousness is marked by high rates of completed suicide, frequent disability, and premature mortality from medical illness. This chapter will review in detail the drugs used for the treatment of bipolar disorder and conclude with recommendations for drug treatments of acute mania, mixed-states, bipolar depression, and rapid-cycling bipolar disorder.
Mania, along with its counterpart melancholia, has been recognized and discussed through the ages. In its purest form, the manic phase of bipolar disorder is one of the most dramatic conditions in all of medicine. Acute mania is easily recognized because it manifests as a dramatic change from usual personality with elevated mood or euphoria, usually mixed with increased activity, excessive talking, and decreased need for sleep. Grandiosity, mistrust, and religious obsession are common psychological symptoms. These psychological and behavioral changes impair judgment that often leads to problematic behaviors and decisions, such as foolish money spending or infidelity. It is not unusual for this changed behavior to lead to serious social, marital, financial, or legal problems. The time course for this change of behavior into the manic state may be gradual over several weeks, or it may be abrupt. Untreated, mania may last weeks to many months. The excess activity and elevated mood of mania is often mixed with irritability, hostility, paranoia, or fluctuations from elation to tearful sadness. This manic pole, thus, is often quite unstable. A significant number of patients experience dysphoric mania, or so-called mixed-states, with mania occurring simultaneously with a major depressive episode. In its extreme form, mania may include psychotic symptoms, such as hallucinations or grandiose delusions, thereby blurring the distinction between acute mania with psychotic features and schizophrenia. Because of this, the definitive diagnosis of bipolar disorder often requires a longitudinal perspective.
The depressed phase of the illness may follow the manic phase or periods of euthymia. While it may be marked by low mood and loss of energy, with patients often taking to the bed and sleeping excessively, it may also be accompanied by subsyndromal symptoms of mania such as racing thoughts and psychomotor agitation. Patients lose self-confidence, become pessimistic, and may consider or attempt suicide during this phase of the illness or during mixed states, often during the transition from mania to depression. In the severe form, the depressed phase may include nihilistic delusions or derogatory auditory hallucinations. The depressed phase of bipolar disorder, unfortunately, frequently accounts for the majority of the ill periods of patient’s lives, and is notoriously difficult to treat. Many patients also suffer chronic subsyndromal depressive symptoms. Some patients presenting with so-called atypical depression may not disclose their periods of hypomania or mania and thus be incorrectly diagnosed with depression rather than bipolar disorder. Interestingly, some patients with early onset and highly recurrent depression may later go on to develop bipolar disorder.
The less severe form of mania, or hypomania, also represents a distinct change in personality with many of the same features as mania, though it does not include psychosis, behavioral changes sufficiently severe to cause hospitalization, or marked impairment in functioning. Patients with hypomania (but never mania) who also suffer depression are characterized as having bipolar II disorder. While not recognized in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV), recent evidence suggests that patients with hypomania may also experience concomitant dysphoric symptoms, or so-called hypomanic-mixed states. Although hypomania may be easy to recognize in person, it is often difficult to diagnose historically, with some patients overendorsing past behaviors and other patients denying obvious past behavioral changes. For this reason, gathering information from family members or other reliable sources is critical in diagnosing past hypomania. For depressed patients, gathering history to elucidate a brief period of elevated mood may be difficult, particularly when the patient has a history of substance abuse or personality disorder. While underdiagnosis of bipolar II disorder is a significant problem, we commonly see an overdiagnosis of bipolar II disorder resulting in long-term medication treatment of a condition that does not exist. Indeed, in many instances, patients are diagnosed with bipolar II disorder when the evidence of past hypomania is scant or better explained by psychosocial factors, impulsive decisions, or substance abuse.
Making the diagnosis of bipolar disorder should not be done lightly because it represents a lifetime condition for which there is only palliative treatment with medications that are often difficult to tolerate. Family and medical history are critical to be sure of the diagnosis. If a person presents with symptoms consistent with mania or hypomania beyond the usual age of onset, in the late teens or early 20s, it is important to look for other causes to explain the change of behavior. Common explanations in younger adults include illicit drugs such as amphetamine or cocaine as well as glucorticoids or anabolic steroids. HIV infections or syphilis may present with manic symptoms in younger persons as well. In older persons presenting with new onset mania, brain infarctions, brain injuries, brain tumors, or autoimmune diseases may lead to manic behaviors. In addition, steroid hormones, antidepressants, or dopamine agonists used to treat Parkinson’s disease may also lead to manic behaviors.
Bipolar disorder is complicated by multiple factors, all of which conspire against successful treatment. Although the vast majority of patients have recurrence of both forms of the illness, a small minority experience recurrent unipolar mania, especially psychotic mania, as the prominent form of their illness. Other patients experience frequent episodes of illness ( four or more times per year), known as rapid cycling, and these patients are frequently treatment resistant. Bipolar disorder is also frequently complicated by co-occurring mental disorders such as anxiety disorders, attention deficit disorder, substance abuse, personality disorders, infectious diseases (e.g., HIV infection), or traumatic brain injuries that result from risky manic behaviors, all of which mitigate against successful treatment. Patients with bipolar disorder also suffer from a number of medical disorders at higher rates than the general population. These disorders complicate treatment and include obesity, diabetes, smoking, chronic obstructive pulmonary disease, HIV infection, hepatitis C, and migraine headaches. Many patients do not adhere to drug treatment because of side effects, denial of illness, or lack of benefit. Finally, the consequences of long-standing bipolar disorder often lead to demoralizing psychosocial problems that make drug treatment alone insufficient for satisfactory outcomes.
Drug treatments must be only part of the treatment of bipolar disorder. A sound therapeutic alliance with the physician and other treatment members is essential for long-term treatment. This alliance will be tested during the times patients experience paranoia and mistrust. Educating the patient and family about the illness and the early manifestations of illness recurrence is critical to prevent full-blown episodes. Most patients can keep mood records and identify stressors as well as subtle behavior changes that suggest other treatments are needed. When possible, family members should be involved to help with early detection of mood changes, medication nonadherence, or substance abuse. Patients also need to learn about the benefits of medication adherence and treatment of medication side effects. Other behavioral strategies, including sleep hygiene, stress reduction techniques, regular exercise, and avoidance of alcohol and illicit drugs should be part of long-term treatment of bipolar disorder. Regular cognitive behavior therapy, social rhythm therapy, or family-focused therapy may prove helpful for patients with bipolar disorder. Some patients may need substance abuse treatment as an ongoing part of their bipolar disorder treatment. Less ill patients may benefit from vocational training.
GENERAL COMMENTS ON THE USE OF MOOD STABILIZERS
The mood stabilizers are a diverse group of drugs used primarily in the treatment of bipolar disorder (manic-depressive illness); as a class, these drugs are effective in acute mania and generally less effective in acute depression, and they act to increase the time to depression or mania recurrence. The longest established mood stabilizers are lithium and the anticonvulsant valproate. Lamotrigine (Lamictal) and all of the second-generation antipsychotic drugs have also shown benefit in different phases of the illness in randomized controlled trials. Clinical trial data are greatest for lithium, divalproex, and the atypical antipsychotics in acute mania. The data are less impressive for bipolar prophylaxis and rather poor for bipolar depression. Unfortunately, no medication is effective in all phases of bipolar disorder. The ideal agent would treat mania and depression in the short term and prevent relapse of either affective phase. This agent, unfortunately, awaits discovery.
A great weight of evidence favors long-term prophylaxis against recurrences after effective treatment of acute episodes. The mainstay of treatment of bipolar disorder for nearly four decades has been lithium. Given its long use, lithium’s efficacy, limitations, and side effects are extremely well documented. Despite less documentation of the benefits and risks of therapy with divalproex, especially for maintenance treatment, it has become widely used, likely based on the perception that it has fewer side effects and greater ease of use than lithium. Therefore, it has become a first-line treatment, although greater overall benefit may still rest with lithium, particularly for suicide prevention. Carbamazepine, lamotrigine, and the atypical antipsychotics have good evidence for treatment of particular aspects of bipolar disorder, though no existing treatment of bipolar disorder is fully satisfactory.
From the distance of the classroom, we often teach our trainees to avoid polypharmacy because of the risk of cumulative side effects and drug interactions. Although a patient with bipolar disorder may require only one agent such as lithium as the mainstay of treatment, over time, given the complexity of bipolar illness, interventions are likely to include the addition of adjunctive treatments, which may include antidepressants, antipsychotics, benzodiazepines, and other compounds. Approximately two thirds of the patients in contemporary studies fail to achieve complete remission or long-term stability on lithium monotherapy.
If possible, one drug should ideally be used as the anchor medication for the disease; for example, a fully unsatisfactory response to lithium for prophylaxis should lead the clinician to consider the use of divalproex or lamotrigine alone. In practice, however, the clinician does not have the luxury of sequential pure trials of the many drugs available. Therefore, unless the initial treatment has yielded no benefit and/or is poorly tolerated, usual practice is to add a second mood stabilizer or second-generation antipsychotic to the ongoing treatment with the first agent while watching for possible interactions. When the goal is monotherapy, this can be done by crosstapering treatment: tapering the first drug and gradually increasing the second.
Bipolar illness is often a severe and life-altering, if not life-threatening, disease and, as with other serious medical conditions (cancer, hypertension, etc.), the clinician should not shrink from using combination therapies. The combined use of the anchor medication (e.g., lithium divalproex, lamotrigine, or a second-generation antipsychotic) and an additional mood stabilizer is recommended when a partial response is achieved with one mood stabilizer. However, controlled studies of each of these combinatorial possibilities have not yet been accomplished. Combination therapy always must be administered with caution, watching for combined toxicities. Some combined regimens are best managed when the clinician monitors blood levels of both compounds.
Over time, the clinician, in partnership with the patient, should be encouraged to reevaluate doses, adverse effects, and regimens, always searching for the optimal combination. Daily mood charting of longitudinal treatment by bipolar patients, with careful documentation of the effect of specific regimens on the various phases of the affective illness, is critical to optimize outcomes.
LITHIUM
Lithium is the lightest solid element in the periodic table; it is active as a psychopharmacologic agent in the form of its singly charged cation. The therapeutic value of lithium was discovered serendipitously by Cade in 1949 when he noted its calming effect on animals. He then tried it on 10 manic patients and found dramatic improvement. The therapeutic usage of lithium was thereafter rapidly explored in Australia and Europe. Its approval for use in the United States, however, was delayed until 1970 because of severe and sometimes fatal cases of lithium poisoning in the 1940s in patients who had unrestricted use of it as a salt substitute. By the time it was approved in the United States, its efficacy as a treatment of mania had been demonstrated beyond question by research in Europe. Its benefit in reducing suicide attempts and completed suicide may be its greatest contribution to the treatment for persons with bipolar disorder.
PHARMACOLOGY
Absorption
Lithium tablets and capsules (Table 4.1) are available as the carbonate salt, which is less irritating to the gastrointestinal tract than the chloride. Each 300-mg tablet contains 8 mmol of lithium. Because lithium is a monovalent ion, 8 mmol is equal to 8 mEq. Lithium is also available as lithium citrate syrup, containing 8 mmol of lithium per 5 mL. Lithium is well absorbed after oral administration. Standard preparations produce peak serum levels in 1.5 to 2.0 hours; slow-release preparations that achieve peak levels in 4.0 to 4.5 hours also are available. No parenteral forms are available.
TABLE 4.1 Common Causes of Secondary Mania
Drug Causes
Central Nervous System Causes
Amphetamine
Traumatic brain injury
Methamphetamine
Meningioma
Cocaine
Glioma (esp right hemisphere)
Antidepressants
Neurosyphilis
Anticholinergics
HIV infection
Hallucinogens
Posttemporal lobectomy
Phenylcyclidine
Epilepsy
Levodopa
Systemic Lupus
Glucocorticoids
Stroke
Anabolic steroids
Multiple sclerosis exacerbation
Blood Levels
Lithium therapy must be guided by measurement of serum levels. Serum level, not oral dose, is highly correlated with both therapeutic and toxic effects. Levels may be reported as milliequivalents per liter or millimoles per liter, or millimolar, which are equivalent because lithium ion is monovalent. Lithium levels are accurately measured by flame photometry or atomic absorption methods that are identical to those used for sodium and potassium. Standards for interpreting serum lithium levels are based on measurement 12 hours after the last oral dose (generally prior to the first morning dose). Regimens in which the entire dose is given at bedtime will produce morning levels 10% to 20% higher than regimens with divided dosing.
Distribution
Lithium distributes throughout total body water, although neuronal levels may be slightly lower than serum levels. There is some lag in penetration into the cerebrospinal fluid, but equilibration between blood and brain occurs within 24 hours. Like sodium, lithium circulates unbound to plasma proteins. In elderly patients, there is a reduction in lean body mass (and thus total body water) by 10% to 15%; thus, lithium has a smaller volume of distribution in elderly patients than in younger patients. This reduction, along with age-related decreases in glomerular filtration rate (GFR), contributes to the need for lower oral doses in elderly patients.
Excretion
Lithium is excreted almost entirely (95%) by the kidney. It is filtered by the glomerulus and, like sodium, it is 70% to 80% reabsorbed in the proximal renal tubules; lithium is also reabsorbed to a lesser extent in the loop of Henle but, unlike sodium, it is not further reabsorbed in the distal tubules. Thus, its excretion is not facilitated by diuretics (e.g., thiazides), which act at the distal tubules. In fact, because proximal reabsorption of lithium and sodium is competitive, a deficiency of sodium, as may be produced by thiazide diuretics, dehydration, or sodium restriction, increases retention of lithium by the proximal nephron and thus increases serum lithium levels. Typically, thiazides increase lithium levels by about 30% to 50%, thus requiring dose reductions in lithium if they are coadministered. On the other hand, the diuretic furosemide, which acts proximally to thiazides in the nephron (at the loop of Henle), apparently blocks lithium reabsorption to an adequate degree so that it does not generally elevate serum lithium levels. Nonetheless, lithium levels must be monitored closely in any patient initiating diuretic therapy.
The renal excretion of lithium is maximal in the first few hours after peak levels are achieved and then proceeds more slowly over several days. In healthy adults, the elimination half-life of lithium is approximately 24 ± 8 hours. Lithium excretion is directly related to GFR. In elderly patients, who have a diminished GFR, the elimination half-life may be significantly prolonged; it also may be increased with renal dysfunction. Conversely, conditions that increase GFR, such as pregnancy, increase lithium clearance.
MECHANISM OF ACTION
Lithium has many known actions in the nervous system at concentrations that approximate the therapeutic serum concentration of 1 mM. Lithium has acute and chronic effects on the release of serotonin and norepinephrine from nerve terminals; at higher concentrations, it has effects on transmembrane ion pumps. Chronic lithium administration has been shown to alter the coupling of a number of neurotransmitter receptors to their signal-transducing G proteins. The two leading candidate mechanisms of lithium action currently are the inositol depletion hypothesis and the action of lithium on the Wnt signaling pathway. Neither of these hypotheses, however, has a direct link to the therapeutic effect of lithium in bipolar disorder been established.
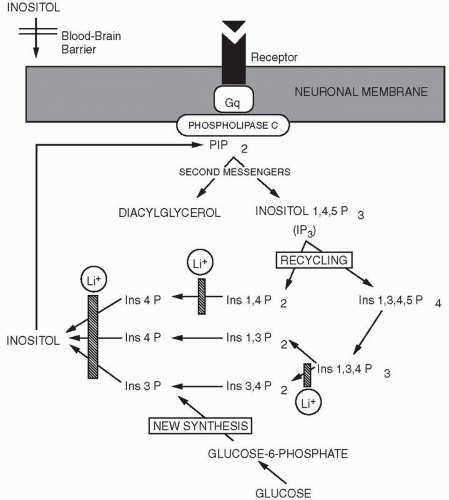
FIGURE 4.1 The effects of lithium (Li+) on the phosphatidylinositol cycle. Lithium blocks the recycling of inositol phosphates and new synthesis of inositol from glucose, thus inhibiting the ability of neurons to generate the second messengers diacylglycerol and inositol 1,4,5-triphosphate (IP3). Gq is the signal-transducing G protein that activates this system. PIP2, phosphatidylinositol 4,5-bisphosphate. (Adapted from Hyman SE, Nestler EJ. The molecular foundations of psychiatry. Washington, DC: American Psychiatric Association, 1993:141.)
Inositol Depletion Hypothesis
Many neurotransmitter receptors (e.g., α1-adrenergic, 5-HT2 serotonin receptors, and muscarinic cholinergic receptors) are linked via the G protein, Gq, to the enzyme phospholipase C, which hydrolyzes the membrane phospholipid phosphatidylinositol 4,5-bisphosphate, to yield two second messengers, diacylglycerol and inositol 1,4,5-triphosphate (Fig. 4.1). Diacylglycerol activates protein kinase C, and inositol 1,4,5-triphosphate binds its receptor on the endoplasmic reticulum to release intracellular Ca2+, itself a critical second messenger. Phosphatidylinositol is synthesized from free inositol and a lipid moiety. Most cells can obtain free inositol directly from the plasma, but neurons cannot, because inositol does not cross the blood-brain barrier. Consequently, neurons must either recycle inositol by dephosphorylating inositol phosphates after they are generated from hydrolysis of phosphatidylinositols or synthesize it de novo from glucose-6-phosphate, a product of glycolysis. Lithium, at therapeutically used concentrations, inhibits inositol monophosphatase (IMPase). This blocks the ability of neurons to generate free inositol from recycled inositol phosphates or glucose-6-phosphate. Lithium-exposed neurons, therefore, have a diminished ability to resynthesize phosphatidylinositol 4,5-bisphosphate after it is hydrolyzed in response to neurotransmitter receptor activation. It has been hypothesized that when firing rates of neurons are abnormally high, lithium-treated neurons will become depleted of phosphatidylinositol 4,5-bisphosphate, and neurotransmission dependent on this second messenger system will be dampened.
However, even if this hypothesis is correct, it remains incomplete. The critical cells in the brain that are targets of lithium’s therapeutic action remain unknown, and it is unclear which of the many phosphatidylinositol-dependent neurotransmitter systems must be dampened for lithium to have its therapeutic effects.
Regulation of the Wnt Pathway and Glycogen Synthase Kinase 3β
In addition to its antimanic effects, lithium has teratogenic effects on embryos of the African clawed toad, Xenopus laevis. Inhibition of IMPase was thought not only to be a candidate mechanism for mood stabilization (as stated previously) but also to explain the dramatic effects of lithium on early development in some model organisms. The teratogenic effects of lithium have now been found to be due not to inhibition of IMPase but to its ability to inhibit the activity of glycogen synthase kinase 3β (GSK-3β). The GSK-3β pathway is a negative regulator of the cellular signaling pathway in which the key intercellular signaling molecule is a peptide called Wnt. Inhibition of Wnt by molecular means reproduces the teratogenic effects of lithium in several species. The possibility that a pathway involved in brain development might also be involved in brain remodeling in response to pharmacologic agents is an intriguing one. Of note, Wnt signaling also interacts with, and is moderated by, trophic factors such as brain-derived neurotrophic factor. Given the continuing difficulty, after more than a decade, of pinpointing a mechanism by which inhibition of IMPase can produce antimanic effects, the implication of GSK-3β has given new impetus to this field.
Lithium Regulation of Adenylyl Cyclase
As mentioned previously, lithium acutely inhibits adenylyl cyclase in most tissues, including those in the brain. Although the concentrations required to exert this effect in the brain appear to be higher than clinically relevant levels, this effect of lithium may account for some of its peripheral side effects. Lithium inhibits the normal activation of adenylyl cyclase by thyroid-stimulating hormone (TSH) and antidiuretic hormone (vasopressin), which may partly explain its antithyroid effects and its tendency to cause defects in the ability to concentrate urine. These effects on adenylyl cyclase may lead to the clinical conditions of hypothyroidism or nephrogenic diabetes insipidus.
Lithium acts also on a protein involved in circadian rhythms. Because the sleep cycle is frequently disrupted in both the depressive and manic phases of bipolar disorder, this property of lithium has been an appealing area of research. Lithium affects a glycogen synthase known as 3β, and this enzyme is involved in circadian rhythms. Recently it was found in vitro that lithium leads to synchronized circadian oscillations by actions on a nuclear receptor known as Rev-erb-α. These studies, though interesting, were performed in cell cultures and further study awaits to determine if this is relevant to unraveling the neurobiologic changes in patients with bipolar disorder.
a8 mEq of lithium is equivalent to 300 mg of lithium carbonate.
INDICATIONS
Lithium has been shown to be effective in bipolar disorder, both for the treatment of acute mania and for prophylaxis against recurrences. Its usefulness in other psychiatric disorders is less well established (Table 4.2).
Bipolar Disorder
Lithium is one of the best-studied and most broadly effective treatments for bipolar disorder. Approximately 50% to 70% of bipolar patients gain at least moderate benefit from lithium during some stage of their treatment. For most patients, however, lithium is not, by itself, a fully adequate treatment for all phases of their illness. Lithium is most effective in the treatment of acute mania and the prophylaxis of manic recurrences, moderately effective in the prophylaxis of depressive recurrences, and generally inadequate as a sole acute treatment of depressive episodes. In each of these situations, lithium may be supplemented by other drugs. During acute manias, supplementation with antipsychotic drugs or benzodiazepines is often beneficial. During acute depressive episodes, supplemental use of antidepressants has become commonplace, although recent data suggest that there is no bene fit to the addition of antidepressants to mood stabilizers in bipolar depression. Bipolar depression is often poorly responsive to all treatments. Because of such complexities, the clinical phases of bipolar disorder are treated separately later.
THERAPEUTIC USE
Before Starting Lithium
Some consensus has developed on the minimum workup of patients prior to starting lithium therapy (Table 4.3). Many clinicians also obtain a pretreatment complete blood count (CBC) because lithium may cause a benign elevation of the white blood cell count. Because lithium may depress sinoatrial node function, patients with sick sinus syndrome probably should be treated only if they have a cardiac pacemaker. There is no need to withhold lithium while waiting for the results of thyroid function tests, because there is no danger to the patient. If the patient proves to have a thyroid abnormality, it can be treated after lithium therapy has commenced. A pretreatment 24-hour creatinine clearance is not needed prior to beginning lithium unless the patient has known renal disease. If a lithium test dose is used for dose prediction and low lithium clearance is discovered or if the patient develops very high lithium levels on low doses when therapy begins, a creatinine clearance should then be performed. Measurement of creatinine clearance is also indicated if during the course of therapy there is a significant increase in the serum creatinine or a significant unexplained increase in lithium levels.
TABLE 4.3 Summary: Method of Lithium Use in Acute Mania
Before beginning lithium
Medical history
Physical examination
Blood urea nitrogen, creatinine
T4, TSH
ECG with rhythm strip recommended if patient is older than 40 years or has history of cardiac disease
CBC (optional)
Human chorionic gonadotropin (pregnancy test), if appropriate
Dosing method
Usually 300 mg two or three times daily. Lower doses in elderly patients or with renal disease (150-300 per day)
Increase by 300 mg every 2 d as tolerated to 900 to 1,500 mg in split doses
Move dose to bedtime with snack once stable
Blood levels
Draw approximately 12 h after the last oral dose 4 to 5 d after starting. At start of therapy, every 5 d to adjust dose
Draw less frequently as levels stabilize
For stable long-term patients, draw every 3-6 mo
Draw immediately if toxicity suspected
Follow-up monitoring (stable patients)
Creatinine, TSH every 6 mo
For patients older than 40 years or with cardiac disease, follow-up ECGs as indicated
Methods have been developed to predict individual dose requirements using a test dose of lithium. In healthy adults, 600 mg can be given and a blood level is drawn 24 hours later. The expected daily dose requirement can be read from a nomogram.
Lower test doses should be used in elderly patients (Table 4.4). This test can be useful in identifying patients who are at the extremes of the dosage range, including some patients with unsuspected renal failure. However, because optimal care requires slow dose increases as side effects allow, dose prediction from a nomogram is no substitute for careful monitoring of side effects and levels.
TABLE 4.4 Prediction of Lithium Dose
Level (mEq/L)
Predicted Total Daily Dose (mg)
<0.05
3,600
0.05-0.09
2,700
0.10-0.14
1,800
0.15-0.19
1,200
0.20-0.23
900
0.24-0.30
600
>0.30
Use with extreme caution
Dosages required to achieve a serum lithium level of 0.9 ± 0.3 mEq/L predicted from a lithium level drawn 24 hours after a single dose of 600 mg.
Adapted from Cooper TB, Simpson GM. The 24-hour lithium level as a prognosticator of dosage requirements: a two-year follow-up study. Am J Psychiatry 1976;133:440.
Prior to starting lithium, patients should be told not to be discouraged if the onset of efficacy is slow and that extra doses are not helpful and may be dangerous. They should also be instructed not to alter their sodium intake, embark on a weight reduction diet, or take diuretics or nonsteroidal antiinflammatory agents (NSAIDs) without medical supervision. This last warning is particularly important now that NSAIDs such as ibuprofen and naproxen are available over the counter.
Blood Levels
Safe and effective lithium therapy is monitored by serum levels; oral dosage is not an adequate guideline. Because lithium levels vary widely from peak to trough with most dosing schedules, it is best to draw blood levels as close to 12 hours after the last oral dose as possible, usually in the morning prior to the first daily dose. This must be emphasized to patients because a misunderstanding will result in confusing or uninterpretable levels. Regimens in which the entire dose is given at bedtime are being used increasingly. These will produce morning levels 10% to 20% higher than regimens using divided dosing.
Because the half-life of lithium is approximately 24 hours and the time to steady state for any drug is four to five half-lives, levels should be drawn no sooner than 5 days after a change in dosage unless toxicity is suspected. Levels drawn before equilibration is complete can be misleading because they may still be on the rise. In elderly patients and in patients with renal disease, the elimination half-life and hence the time to equilibration is prolonged (often 7 days or more). If toxicity is suspected, lithium should be withheld and a level determined immediately. Interpretation of the level requires that the time since the last dose be taken into account.
Using Lithium
In healthy adults, the usual starting dosage is 300 mg three times daily, but smaller dosages (e.g., 150 mg twice daily) should be used if the patient is elderly or has renal disease, and in less acute circumstances some clinicians will begin at smaller doses in other patients to maximize tolerability initially. At the beginning of therapy, it is useful to draw levels after 5 days and to use results to adjust the dosage upward to the therapeutic range; dosage prediction nomograms, although available, are rarely used. Once the patient is stable, the whole dose can be given at bedtime.
Many side effects that occur early in therapy, such as nausea and tremor, are associated with absolute levels but also may occur at lower levels of lithium if the levels are rising too rapidly. It is best to increase the dosage slowly to avoid such side effects and to maximize patient comfort and eventual compliance. If troublesome side effects emerge at the beginning of therapy, the oral dosage should be temporarily decreased and then slowly increased again after several days as side effects allow. If there is pressure to obtain rapid symptom control, temporary use of antipsychotics or benzodiazepines may be more expedient.
Dosage Forms and Dosing Intervals
One of the major problems with long-term lithium therapy is patient compliance. Compliance is clearly improved when dosing regimens are simplified. Most patients tolerate lithium well on a twice-daily regimen, allowing omission of the often forgotten midday dose. Indeed, there is evidence that lithium may be best tolerated by the kidney in a single nightly dose. Patients taking a single daily dose have less polyuria and fewer renal structural abnormalities than patients taking multiple daily doses (see later section on renal effects). The data suggest that the kidney is able to tolerate higher peak levels reached with single daily dosing but benefits from lower troughs. From the current evidence, it would appear appropriate to treat patients with single daily doses, especially if they have compliance problems or severe polyuria. In any case, there appears to be no reason to give lithium more frequently than twice daily unless the patient has serious peak level side effects. Slow-release lithium may help patients who have side effects at peak levels such as severe tremor or nausea, but a minority of patients will only tolerate lithium on a regimen of smaller, more frequent daily doses. The slow-release preparations available in the United States have excellent bioavailability and result in less dose fluctuation during the day than standard lithium. Because their absorption is delayed, however, these preparations have a greater tendency to cause diarrhea than regular lithium preparations.
Target Plasma Levels
As described previously, regimens in which the entire dose is given at bedtime will produce morning levels 10% to 20% higher than regimens with divided dosing. The target levels described in this section are based on divided dosing regimens. For acute mania, a therapeutic response is usually achieved at serum levels of 0.8 to 1.0 mM. There is no convincing justification for levels beyond 1.2 mM; levels greater than 1.5 mM are likely to be toxic. The oral dose that produces therapeutic levels varies with the size of the patient and his or her GFR. In healthy adults, the typical oral dose to produce a level of 1.0 mMis in the range of 1,500 ± 300 mg, but extreme doses range from 300 to 3,000 mg. Some clinicians report that early in the treatment of acute mania the oral doses needed to produce a given level may be higher than later in the treatment. The reasons for this clinical observation are unknown. For prophylaxis, levels of 0.8 to 1.0 mM have been suggested to be more effective than lower blood levels, although they result in more side effects. If side effects are severe and may compromise therapy, the lowest effective serum level for that patient should be determined empirically. If a patient cannot tolerate lithium in the therapeutic range, substitution of another mood stabilizer should be considered.
Monitoring Long-Term Therapy
Following initiation of lithium therapy, patients should have a follow-up serum creatinine drawn after reaching a therapeutic blood level. Follow-up electrocardiograms (ECGs) should be performed as clinically indicated. Lithium can be expected to cause a variety of benign changes in the ECG, including a pattern similar to that of hypokalemia. (It is important to make sure that the patient is not, in fact, hypokalemic.) Therapy should be interrupted only if a potentially dangerous arrhythmia emerges.
During long-term lithium use, serum levels for stable patients can be obtained yearly as indicated (more frequently if toxicity is suspected, if noncompliance is a problem, if medications that affect lithium levels are used, or if mood symptoms emerge). Serum creatinine and TSH should be drawn every 6 to 12 months or if signs of renal or thyroid toxicity emerge. An unexplained increase in serum lithium levels requires an investigation of renal function.
Discontinuation of Lithium Therapy
Both open and controlled trials have documented that there is a substantial risk of new episodes of mania or depression following discontinuation of lithium, or rapid lithium dose change, even after years of stability on lithium. A review of existing studies found a high early risk of recurrent manias in bipolar patients following relatively abrupt lithium discontinuation, with over half of the recurrences occurring within the first 3 months after discontinuation. Depressive recurrences tended to come later. More striking, the survival time for 50% recurrence was 5 months, far shorter than during lithium treatment and even shorter than in previous untreated cycles (11.6 months) (Suppes et al., 1991). These data suggest a rebound effect with rapid discontinuation. In a prospective study, this group found that gradual (2 to 4 weeks) discontinuation of lithium diminished the risk of early recurrence. Given these data, it would be prudent to taper lithium no more rapidly than 300 mg per month, unless side effects demand a more rapid taper. Concern also has been raised that discontinuation of lithium may cause later unresponsiveness to lithium. However, no evidence of such lithium resistance has emerged in recent follow-up analyses.
USE IN PREGNANCY
Women with bipolar disorder may experience significant affective symptoms during pregnancy and are at elevated risk of developing postpartum manias or depressions. However, use of lithium, divalproex, lamotrigine, or carbamazepine during the first trimester of pregnancy is associated with increased risk of major birth defects. All women with bipolar disorder considering pregnancy or who become pregnant should receive counseling on the relative risks of pharmacologic treatment versus no treatment in their particular case. A contingency plan should be made (and discussed with the family) concerning a course of action, should a severe episode occur, especially during the first trimester of pregnancy.
Use of lithium during the first trimester has been associated with risk of Ebstein’s anomaly (right ventricular hypoplasia and tricuspid valve insufficiency). Recent epidemiologic and case-control studies suggest that the rates in the original Lithium Register were likely overestimates due to an overreporting bias. Although there does appear to be an association (with a risk in the general population estimated at 1 in 20,000 births) between first-trimester lithium exposure and risk of Ebstein’s anomaly, the revised estimate is about 1 in 2,000 for exposure, a 10-fold increase over the general population. Thus, the absolute risk is low and certainly does not itself justify a recommendation of termination of pregnancy. Furthermore, modern sensitive fetal ultrasound technology can detect the presence or absence of Ebstein’s anomaly by week 16 of gestation. Because of the risks posed by all mood stabilizers, electroconvulsive therapy (ECT) is the treatment of choice for severe manic or depressed episodes. Alternatives that appear to be safer than lithium, divalproex, or carbamazepine include high-potency antipsychotic drugs and benzodiazepines.
Lithium use later in pregnancy may pose potential complications for the mother. Regulation of the lithium level may be complicated by changes in maternal blood volume, which increases during pregnancy by 50%, and GFR, which increases by 30% to 50%. At parturition, diuresis may lead to shifts in plasma lithium levels, which must be monitored to avoid lithium toxicity. In addition, therapeutic lithium levels at parturition are associated with significant symptoms in the neonate, but dose reduction of lithium immediately prior to delivery may prevent this.
Lithium is secreted in breast milk at about half the serum levels in the mother. The effects of lithium on growth and development are unknown. Therefore, breast-feeding is typically discouraged among mothers who take lithium to reduce the risk of postpartum illness.
Despite the risks associated with lithium use during pregnancy, they must be balanced against the risks of untreated or undertreated bipolar disorder to both mother and fetus. A recent prospective study suggests that the risk of relapse, especially to depression or dysphoric states was double in those who stopped mood stabilizers. In addition, the time to mood recurrence was fourfold shorter, and the time spent ill during pregnancy was five times more in those who stopped mood stabilizers than in those who continued them. Thus, stopping mood stabilizers is risky, and medications such as lithium are reasonably continued during pregnancy after a careful presentation to the patient and family of the risks and benefits.
USE IN ELDERLY PATIENTS
Given the decrease in GFR and the decreased ratio of water to fat that occurs with increasing age, several precautions should be taken when using lithium in elderly patients. Elderly patients should be started at lower dosages (e.g., 150 to 300 mg twice daily) depending on age and presence of renal dysfunction. Level drawing and dose changing should be slower to reflect the increased time to steady state (>7 days). In addition, the physician must be aware of any underlying cardiac disease. Elderly patients are often on drugs, such as diuretics and NSAIDs, that may predispose to lithium toxicity. Finally, elderly patients are more sensitive to the neurologic toxicity of lithium. The physician should carefully document the patient’s cognitive function before beginning lithium and then monitor the patient for the emergence of subtle confusional states. Risks of producing confusional states are greater if the patient is on combined therapy with other drugs such as antidepressants, antipsychotics, anticonvulsants, or anticholinergics.
SIDE EFFECTS
Use of lithium is complicated by its low therapeutic index. At serum levels not much higher than therapeutic levels, significant toxicity may occur. Even at therapeutic levels, perhaps 80% of the patients experience some side effects, although only 30% would be characterized as moderate or severe. Mild to moderate side effects can be bothersome enough to patients to limit therapy. The most common side effects include thirst, increased urination, tremor, and weight gain. Side effects are often a particular problem at the initiation of therapy when levels are rising or several hours after dosing when peak levels are achieved. Patients who develop bothersome side effects within several hours of a dose may do better on a slow-release preparation; alternatively, the dosage schedule can be altered so that the medication is administered in more frequent smaller doses, but multiple daily dosing makes compliance more difficult.
As serum levels increase, more serious toxic symptoms can be expected, but because patients have varying susceptibility, lithium toxicity is primarily a clinical diagnosis for which serum levels provide confirmation. In general, some toxicity is to be expected at levels above 1.5 mM. Severe toxicity may manifest at levels as low as 2.0 mM and is almost always evident at levels above 3.0 mM. In addition to its dose-related toxicities, lithium may produce several idiosyncratic reactions, such as dermatologic reactions, which may occur at any level.
Gastrointestinal Side Effects
Patients treated with lithium may experience nausea, vomiting, anorexia, diarrhea, or abdominal pain. These symptoms are dose related, emerging at higher serum levels or with rapidly increasing serum levels at the initiation of treatment even if the actual level is not high. Thus, these symptoms are common at the start of treatment and are usually transient. If they occur with rising levels at the start of treatment, the dosage can be temporarily decreased and then increased again more slowly when the symptoms abate. Nausea may be minimized if lithium is given with meals or if slow-release preparations are used. In some cases, cotreatment with a histamine-2 (H2)-blocker is also helpful in improving tolerability. However, slow-release preparations may result in a higher incidence of diarrhea than regular lithium. Patients who do not tolerate either preparation of the carbonate salt may have less gastrointestinal distress with lithium citrate syrup. Gastrointestinal symptoms that emerge late in treatment suggest the presence of toxic drug levels.
Renal Effects
Although lithium commonly causes defects in urine concentration ability, it rarely causes renal failure in patients whose lithium levels are maintained in the therapeutic range. An early report of serious abnormalities, including glomerulosclerosis and interstitial fibrosis on renal biopsies of patients on long-term lithium therapy, however, raised the concern that long-term lithium therapy might lead to renal failure. Longitudinal studies have failed to confirm this fear and have not offered comparable reassurance for patients who have had periods of significant lithium toxicity. In a naturalistic study, 46 patients who had taken lithium for a mean of 8 years were compared with 16 patients undergoing renal biopsies for other reasons. The number of sclerotic tubules and atrophic glomeruli in the lithium-treated patients were slightly higher than those in controls, but the differences did not achieve statistical significance; changes in glomerular function were not clinically significant. However, the proportion of sclerotic glomeruli and atrophic tubules among lithium-treated patients was higher in patients who received lithium in divided daily doses than in those patients taking once-daily dosing.
Polyuria
The most common renal problem due to lithium therapy is polyuria. This may be partly due to the antagonistic effect of lithium on the renal actions of antidiuretic hormone, leading to an inability to produce appropriately concentrated urine; however, other renal processes may contribute. Polyuria may occur in 50% to 70% of the patients receiving long-term therapeutic doses of lithium; about 10% have a urine output greater than 3 L per day, thus qualifying as having nephrogenic diabetes insipidus. Currently, lithium therapy is the most common cause of nephrogenic diabetes insipidus. Whether polyuria progresses with duration of therapy is unclear. One study of 32 patients taking lithium for an average of 10 years found no interval change in polyuria in the final 2-year period of follow-up. Polyuria, nocturia, and thirst can be very troublesome to patients. When severe, these symptoms may interfere with normal living habits and sleep. These symptoms may improve with dosage reduction and usually abate entirely when lithium is discontinued. A small number of patients, however, seem to have long-term (many months) or permanent urine-concentrating defects that suggest structural damage to the kidney.
Management of Polyuria. Patients who are symptomatic from polyuria should first be established at the minimum effective lithium levels for them. Second, lithium can be administered as a single bedtime dose. Third, diuretics can be administered, because diuretics paradoxically decrease urine outputs in lithium-induced polyuria.
The potassium-sparing diuretic amiloride markedly decreases urine volumes without a major effect on lithium or potassium serum levels, so long as the patient has normal renal function. Amiloride is started at 5 mg twice daily and can be increased to as much as 10 mg twice daily if the effect is inadequate. Total dosages above 20 mg per day do not have an added benefit. With amiloride, patients can remain on normal diets with unrestricted sodium. Nonetheless, it is prudent to monitor weekly lithium and potassium levels for several weeks after beginning amiloride to be sure that there are no changes.
Should amiloride not be tolerated, hydrochlorothiazide, 50 mg per day, can be substituted; should amiloride be tolerated but prove inadequately effective, hydrochlorothiazide, 50 mg per day, can be added. However, it must be recalled that thiazides alone or in combination with amiloride may increase lithium levels substantially. Thiazide diuretics reduce extracellular volume, leading to a compensatory increase in sodium reabsorption, thereby producing increased lithium reabsorption and elevation of lithium levels. Typically, thiazides used alone increase lithium levels by 30% to 50%. Thus, if thiazides are used with or without amiloride, the lithium dosage should initially be halved and lithium levels monitored weekly; the needed oral dose to achieve the patient’s therapeutic blood level can then be established. Thiazides have the additional problem of causing potassium depletion; even if the patient is also taking amiloride, potassium levels should be monitored, initially on a weekly basis, until it is determined whether the patient is wasting potassium and needs potassium supplementation. When patients are taking diuretics, it is prudent to obtain potassium levels when lithium levels are drawn.
Other Renal Problems
Rarely, patients have an acute increase in serum creatinine with the institution of lithium therapy, usually with a benign urinalysis (i.e., no cells or casts). Such cases are more common than is reported in the literature. These patients generally do not require a diagnostic renal biopsy. Most patients have interstitial nephritis (tubulointerstitial nephropathy). In general, when the creatinine increases significantly in the context of lithium therapy, lithium should be discontinued and a 24-hour creatinine clearance should be performed. Of course, the physician should be sure that the problem is not due to an episode of lithium toxicity, dehydration, obstruction, or the addition of another medication. Patients who have acute interstitial nephritis will have markedly decreased creatinine clearance. Fortunately, when these changes are detected early, they are reversible with permanent discontinuation of lithium.
A small number of patients have been reported to develop nephrotic syndrome in association with lithium therapy. Nephrotic syndrome is usually reversed by discontinuation of lithium, but occasionally corticosteroids have proved necessary. Renal biopsies have revealed fusion of renal epithelial foot processes (minimal change disease). These patients should not be treated with lithium again.
Edema
A minority of patients develop intermittent edema of the lower extremities or face, unrelated to any changes in renal function. The edema often resolves spontaneously. If a medical etiology has been ruled out and the edema poses a problem for the individual, lithium-related edema can be treated with the diuretic spironolactone. If spironolactone is administered, lithium levels and electrolytes should be monitored (lithium levels may increase with the use of this drug).
Neurologic Side Effects
Mild neurologic side effects may occur with increasing lithium levels at the start of therapy or with stable therapy, especially at times of peak levels. These complaints include lethargy, fatigue, weakness, and action tremor. The tremor is a 7- to 16-Hz action tremor similar to physiologic or essential tremor and unlike the pill-rolling tremor of parkinsonism. It is aggravated by anxiety and performance of fine motor movements. It also may be aggravated in some patients by concomitant administration of antidepressants. Tremor may be embarrassing for some patients and may impair normal daily activities involving delicate motor movements. Tremor can often be controlled by decreasing the lithium dosage, if possible, and decreasing or stopping caffeine intake and, if these maneuvers fail, by adding a β-adrenergic blocker, such as propranolol. Propranolol, 10 to 20 mg, can be taken 30 minutes prior to an activity in which tremor will be a serious problem. For patients who require suppression of tremor all day, propranolol may be started at 10 to 20 mg twice daily with the dose titrated upward as needed. Patients who develop central nervous system side effects from propranolol may do better on the less lipophilic drug atenolol, 50 mg per day in a single daily dose. Coarsening of the tremor may be a sign of lithium toxicity.
Lithium may independently cause extrapyramidal symptoms (EPS) in a very small minority of patients and may worsen neuroleptic-induced EPS in some patients. The balance of the evidence suggests that lithium neither prevents nor predisposes to tardive dyskinesia (TD). There have been case reports of lithium causing recurrence of neuroleptic malignant syndrome (NMS) when used in place of antipsychotic drugs in patients recovering from NMS. This may be due to the same mechanisms by which lithium causes EPS. Given the rarity of such reports, lithium may be used safely in patients who have recovered from NMS, but the possibility of recurrence should be kept in mind.
Several cases of benign intracranial hypertension (pseudotumor cerebri) occurring in association with lithium therapy have been reported. Patients presented with headache, blurred vision, and papilledema. If lithium is causally related to pseudotumor at all (perhaps by inhibiting cerebrospinal fluid reabsorption), the problem appears to be extremely rare. Therefore, screening funduscopic examinations appear to be unnecessary. However, it would be prudent to perform a funduscopic examination and to consider this diagnosis in patients who complain of severe headaches or new visual abnormalities while on lithium.
Lithium may produce electroencephalographic changes in a large proportion of patients, but only variable and minor effects on seizure threshold have been reported. Although worsening has been reported in some patients with complex partial (temporolimbic) epilepsy, many other such patients have improved behaviorally without a worsening pattern of seizures. In an open study of bipolar patients with seizure disorders (primary generalized seizures or complex partial seizures), lithium was effective in treating the mood disorder and did not increase the seizure frequency in patients with active seizures or induce seizures in patients whose seizures had remitted (Shukla et al., 1988). Pending new data, lithium should not be withheld from patients who have both mood and seizure disorders, but careful clinical monitoring is needed. Lithium does not affect serum levels of anticonvulsants.
The appearance of new neurologic symptoms during the course of therapy, even if mild, should raise the suspicion of lithium toxicity. A lithium level should be drawn and subsequent doses withheld until the question of toxicity is resolved. Patients may develop moderately severe neurologic symptoms at lithium levels not much higher than therapeutic ones. Some elderly patients or patients with brain lesions or dementia may develop such toxic symptoms even in the conventional therapeutic range. Moderate neurologic toxicity includes neuromuscular irritability, including twitching and fasciculations, EPS, ataxia, coarsening of tremor, dysarthria, incoordination, difficulty in concentrating, confusion, visual disturbance, and altered levels of consciousness. Symptoms of encephalopathy due to lithium, such as confusion or hallucinations, may be difficult to distinguish from the underlying illness, especially in patients who have a concomitant dementia. Lithium combinations with second-generation antipsychotics (commonly used in mania) are more likely to produce EPS and encephalopathy than either drug alone.
Severe neurologic toxicity can cause ataxia, seizures, hallucinations, delirium, coma, and death. With lithium poisoning, permanent memory impairment, nystagmus, and cerebellar ataxia may occur.
Cognitive and Psychological Side Effects
Patients taking lithium may complain of dull affect, a sense of depersonalization, a general “graying” of their mental life, or loss of creativity. Patients also may complain of memory disturbance and cognitive slowing. It has been difficult to quantify these complaints, some of which may reflect loss of valued hypomanias or mild depression. Schou (1984) followed artists taking lithium and found that creativity increased, decreased, or was unchanged with lithium treatment, depending on the individual. Several investigators have found that subjective complaints of memory disturbance in their study population were partly explained as effects of aging and depression, although lithium could not be completely exonerated from impairing certain cognitive tasks. Joffe et al. (1988) tested attention, concentration, visuomotor function, and memory in 12 normal controls and 18 patients taking lithium (serum levels 0.7 to 0.9 mM) and on carbamazepine. The lithium and carbamazepine patients did not differ from controls. Further study with larger sample sizes is necessary to decide this issue. Presently, when patients complain of such side effects it makes sense to attempt prophylaxis with the lowest possible lithium level that affords effective treatment. When patients complain of cognitive difficulty, a mental status examination should be performed and symptoms of depression should be elicited to rule out a treatable condition. In some cases, alternative therapies, such as an anticonvulsant, will be necessary.
Thyroid Side Effects
Lithium interferes with the production of thyroid hormones at multiple steps, including iodine uptake, tyrosine iodination, and release of T3 and T4. Inhibition of the TSH-responsive adenylyl cyclase in thyroid cells may be responsible. Clinically, patients may develop goiter with or without some degree of hypothyroidism. Overall, approximately 5% of patients receiving long-term lithium therapy develop hypothyroidism (compared with 0.3% to 1.3% in the general population, predominantly women). Perhaps 3% of patients taking lithium will develop goiter. On the other hand, a much larger percentage develops increased levels of TSH. The clinical importance of this latter finding is not clear; treatment of TSH abnormalities in the absence of abnormalities in T3 or T4 is controversial. Patients with antithyroid antibodies prior to onset of lithium therapy appear to be at higher risk for development of hypothyroidism. The timing of onset of thyroid problems during lithium therapy is extremely variable.
Because of lithium’s thyroid toxicities, it is important to perform baseline thyroid studies (TSH, T4). In follow-up, patients should be observed for development of goiter, and thyroid function tests (at least a TSH, which is the most sensitive for hypothyroidism) should be done every 6 months. Development of thyroid abnormalities does not necessitate a change in lithium therapy but rather treatment of the thyroid problem, usually in consultation with an endocrinologist or general internist. Should hypothyroidism or goiter develop, it can generally be treated by the addition of thyroid hormone (e.g., synthetic T4). Because hypothyroidism, including lithium-induced hypothyroidism, can present as refractory depression (Yassa et al., 1988), it is important to check thyroid function if the patient’s pattern of depressive episodes changes in character or becomes treatment resistant.
Cardiac Toxicity
It is reasonable to question patients about cardiac symptoms or history of cardiac disease before initiating lithium therapy. Patients older than 50 years or those who have a cardiac history should have a baseline ECG with follow-up ECGs as clinically indicated. If there is any question about cardiac disease, a consultation with an internist should be obtained. During follow-up visits, patients should be asked about dizziness, palpitations, or irregular heartbeats when they are asked about other possible side effects of lithium.
Many patients treated with lithium develop ECG changes such as T-wave flattening or inversion. These changes correlate poorly with serum levels, are reversible with discontinuation of lithium, and are almost always benign. It is important, however, that other possible causes of T-wave abnormalities, such as hypokalemia, are not ignored because the patient is taking lithium.
Arrhythmias due to lithium have been described, almost always in patients with preexisting cardiac disease. Sinoatrial node dysfunctions, including sinoatrial block and tachycardia, have been reported. These may present with dizziness, syncope, or palpitations or may be asymptomatic. They are reversible with discontinuation of lithium. Patients with preexisting sinoatrial node dysfunction (sick sinus syndrome) can only be safely treated if they have a cardiac pacemaker. Because the calcium channel blocker verapamil is occasionally used as a treatment of bipolar disorder, there is a possibility that it will be used together with lithium. Cases of serious bradycardia with this combination have been reported.
Ventricular arrhythmias also have been reported, although rarely. In several case reports, patients were also receiving antipsychotic drugs. Now that it is known that some antipsychotics (e.g., thioridazine and trifluoperazine) are calcium antagonists, it is possible that the cause for the arrhythmias should be reassigned to the antipsychotic or to combined toxicity.
Dermatologic Reactions
Dermatologic reactions appear to be idiosyncratic rather than dose related. They include acne and psoriasis (which are the most frequent), maculopapular eruptions, folliculitis, and extremely rare cases of exfoliative dermatitis. This last, a presumed hypersensitivity reaction, may be life threatening; patients who recover should not receive lithium again.
Acne
Acneiform eruptions are probably the most common dermatologic reaction to lithium. They may prove to be a major obstacle to acceptance of lithium by adolescents and young adults unless vigorously treated. The acne usually begins as a monomorphic eruption (all lesions in the same stage) and may occur on the face, neck, shoulders, and back. The eruptions may be new or an exacerbation of preexisting acne. The acne usually responds to vigorous treatment with standard antiacne regimens. If the acne does not respond, a dermatologic consultation might be useful, especially if lithium refusal could result from the patient’s cosmetic concerns.
Psoriasis
Lithium may cause exacerbations of preexisting psoriasis or onset of new psoriasis. Psoriasis due to lithium tends to be treatment resistant but usually regresses with discontinuation of the drug. The decision to stop lithium must obviously be balanced with the risks to the patient from affective illness. The anticonvulsants do not appear to have any effects on this skin disorder. The condition of some patients with preexisting psoriasis do not worsen on lithium; thus, a history of psoriasis is not an absolute contraindication to lithium therapy, although patients with severe disease or psoriatic arthritis might be more safely treated with anticonvulsants, including divalproex, carbamazepine, gabapentin, or lamotrigine.
Other Dermatologic Reactions
Maculopapular rashes (usually pruritic) have been reported to occur occasionally early in treatment. These often regress by themselves. Asymptomatic folliculitis, which may occur as hyperkeratotic erythematous follicular papules on extensor surfaces, the abdomen, and the buttocks, has also been reported. It appears to pose little problem for patients and should not require changes in lithium therapy.
Hair loss is a rare side effect of lithium therapy. When hair loss occurs, it is important to check for hypothyroidism and other possible causes of alopecia.
Hematologic Effects
Lithium produces a benign, relative leukocytosis, increasing neutrophil mass without impairing function. There is no known adverse effect; in fact, leukocytosis induced by lithium has been exploited in the treatment of leukopenic patients. It is important to be aware of this effect of lithium to avoid unnecessary medical workups for elevated white blood cell counts. The total white blood cell count rarely exceeds 15,000/µL as a result of lithium therapy alone.
Weight Gain
A side effect that can be extremely troublesome and lead to noncompliance or lithium refusal is weight gain. In some studies, lithium has been associated with weight gain of more than 10 kg in 20% of patients on long-term therapy. Lithium has been reported to have insulin-like effects on carbohydrate metabolism. Antipsychotic drugs and cyclic antidepressants also may cause obesity (a hypothalamic mechanism has been the hypothesized cause for this). Patients who are polyuric should be advised not to replace their fluid losses with high-calorie beverages such as beer or sugary sodas. Some will benefit from dietary consultation. For some patients who have developed severe obesity, substitution of another drug, such as aripiprazole, for lithium might be considered.
Calcium Metabolism
Anecdotal reports and several small studies have associated lithium therapy with mild elevations in calcium and parathyroid hormone. These elevations appear to be rarely, if ever, clinically significant. However, because alterations in calcium level are associated with neuropsychiatric symptoms, serum calcium levels might be obtained if there is a change in a patient’s pattern of symptoms, especially depressive symptoms.
EVALUATION AND TREATMENT OF LITHIUM TOXICITY DUE TO ELEVATED LEVELS
For mild toxicity, lithium should be withheld until levels return to the patient’s usual therapeutic range. If an obvious cause for the change in level cannot be found, a renal workup should be undertaken, including urinalysis and creatinine clearance.
For moderate to severe lithium toxicity, the patient is best admitted to a hospital. Adequate sodium should be given, and lithium levels should be checked several times a day to make sure that they are decreasing. If the patient does not have congestive heart failure or renal failure, intravenous administration of normal saline at a rate of 150 to 200 mL per hour is often effective in reducing lithium levels rapidly; this is safe as long as urine output is adequate.
Acute Lithium Intoxication
Acute lithium intoxication, manifested by a severe clinical syndrome or levels above 3.0 mEq/L, is a medical emergency. Because the severity and reversibility of toxic symptoms are related both to the serum level and to the duration of high levels, rapid aggressive treatment is necessary even if the patient appears clinically well. Indeed, early in lithium poisoning the patient’s symptoms may be relatively mild despite high levels, giving the physician a false sense of security. Symptoms of serious intoxication include both systemic and neurologic symptoms, including nausea, vomiting, diarrhea, renal failure, neuromuscular irritability or flaccidity, ataxia, dysarthria, coarse tremor, confusion, delirium, hallucinations, seizures, and stupor. Protracted coma and glucose intolerance have been reported. Lithium poisoning also may cause death. Survivors of serious toxicity may suffer permanent cerebellar ataxia and severe permanent anterograde amnesia.
In treating acute lithium intoxication, the therapeutic goal is to remove lithium from the body as rapidly as possible. It is important to obtain a toxic screen to know what other agents the patient has ingested, especially if the case appears to be an intentional overdose. If the patient is stuporous or comatose, protection of the airway, with intubation if necessary, and cardiorespiratory support should be the first priority. In overdose cases in which the drug was taken less than 4 hours prior to treatment, induction of vomiting in alert patients or gastric lavage in comatose patients will help diminish the risk of worsening toxicity. Because lithium levels are often high in gastric secretions, continuous gastric aspiration can be helpful.
Despite the fact that most reports of lithium intoxication are either anecdotal or retrospective, there seems to be strong evidence that management should be aggressive. If lithium levels are less than 3 mM and signs of intoxication are mild, fluid and electrolyte abnormalities should be corrected and normal saline may be administered at a rate of 150 to 200 mL per hour, as long as urine output is adequate. If the lithium level is greater than 3 mM and signs of toxicity are severe, or if there is poor urine output or renal failure, prompt institution of dialysis is indicated. If the lithium level is above 4 mM
Only gold members can continue reading. Log In or Register to continue