Dynamic MRI Using the Upright or Positional MRI Scanner
F. W. Smith
M. H. Pope
D. Wardlaw
Clinical symptoms in many spinal syndromes such as lumbar spinal stenosis are posture related. Pain and numbness in the buttock and leg are provoked either by walking or by prolonged standing. On the contrary, lying and sitting can obtain symptomatic relief. Not only spinal canal area but also intervertebral foraminal space can decrease with extension (1). The nerve root is constrained in the intervertebral foramen (IVF) and may be easily compressed or mechanically irritated under unfavorable conditions of degeneration and movement.
FINDINGS OF PREVIOUS STUDIES
Kinematic Change of Intervertebral Foramen
Panjabi et al. (1) performed an in vitro study providing data about the three-dimensional movements of the IVF. In nondegenerated specimen, the average height, width, and area of the IVF were 20.9 mm, 10.2 mm, and 185.0 mm. The height of the IVF increases about 7% during flexion and decreases about 6% decrease during extension. The width of the IVF increases about 15% during flexion and decreases about 12% decrease during extension.
Nowicki et al. (2) examined cadaveric lumbar motion segments with computed tomography (CT) and magnetic resonance imaging (MRI). They examined the effect of extension, flexion, lateral bending, and axial rotation on the anatomical relationship of the spinal nerves in the neural foramen to the ligamentum flavum and the intervertebral disc. The neural foramina were classified as having no evident stenosis, as being stenotic, as having occult stenosis, or as showing resolved stenosis on the basis of the images and sections before and after loading. Extension loading produced the most cases of nerve root contact. Nowicki et al. demonstrated intermittent stenosis of the neural foramina.
Axial Loading of the Spine in Patients with Lumbar Spinal Stenosis
To determine the mechanical effects on the lumbar spinal canal in a simulated upright position, Willen et al. used a portable device for axial loading of the lumbar spine in CT and MRI (3). They found a statistically significant reduction of the dural sac cross-sectional area in at least one site during axial compression. Narrowing of the lateral recess and deformation of nerve roots could be estimated in the MRI study but not measured.
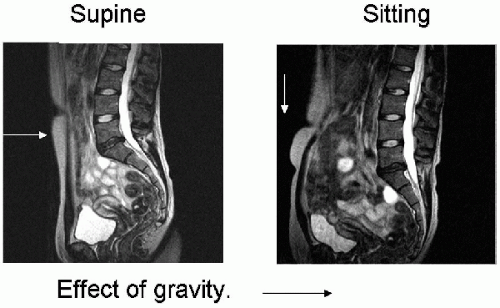 FIG. 8.1. Effect of gravity: supine versus erect. |
Positional MRI
A newly developed positional MRI (pMRI) machine (Indomitable from FONAR) allows patients to simply walk in and be scanned while standing up and sitting down. Using this MRI, we can get the image of lumbar standing position, flexion, and extension position. The new stand-up MRI machine at the University of Aberdeen allows patients to walk in and be scanned while lying down, standing up, or sitting down. The gravity vector is roughly parallel to the spine in the erect or seated posture rather than at right angles in the supine posture. This changes the configuration of the spine (Fig. 8.1). The signs and symptoms of much of spinal conditions (i.e., spinal stenosis) are often posture related.
Jinkins and Dworkin (4) demonstrated the general utility of the pMRI unit in enabling upright, weight-bearing positional evaluation of the spinal column during various dynamic-kinetic maneuvres in patients with degenerative conditions of spine.
Intervertebral Relationships and Lumbar Posture
The study reported below was performed to assess the relationship between intervertebral relationships and lumbar posture in patients using pMRI.
Materials and Methods
Subjects
Related posts:
 Biomechanics of Spondylolysis with Reference to its Etiology, Diagnosis, Treatment, and Slippage
Biomechanics of Spondylolysis with Reference to its Etiology, Diagnosis, Treatment, and Slippage
 Mechanics of Neurological Impingement
Mechanics of Neurological Impingement
 Sport, Spondylolysis, and Spondylolisthesis
Sport, Spondylolysis, and Spondylolisthesis
 Direct Repair of the Pars Interarticularis for Spondylolysis
Direct Repair of the Pars Interarticularis for Spondylolysis
 Posterior Lumbar Interbody Fusion (PLIF) in Spondylolisthesis
Posterior Lumbar Interbody Fusion (PLIF) in Spondylolisthesis
 Bone Graft Alternatives in Spinal Surgery
Bone Graft Alternatives in Spinal Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


