Newborns have a polyphasic sleep pattern and spend about two-thirds of their time sleeping during the first weeks of life. This polyphasic sleep pattern gradually changes into the monophasic adult pattern (1). Brain electrical activity, body and eye movements, and respiratory patterns are used to differentiate sleep and wake states (see Tables 2-1 and 2-2). On falling asleep, a normal newborn enters into rapid eye movement (REM) sleep, also referred to as active sleep. Random spontaneous movements of arms, legs, and facial muscles accompany active sleep. In premature infants (<37 weeks conceptional age [CA]), it can be difficult to distinguish REM from wakefulness. Body movements and brain stem electrical activity are present at approximately 10 weeks CA, and cerebral cortical activity can be identified at 17 weeks CA. Rhythmic cycling body movements begins at 20 to 24 weeks CA. High-voltage slow (HVS) waves and low-voltage (8-14 Hz) activity are separated by 20- to 30-second intervals of low-voltage nearly isoelectric background. This electroencephalography (EEG) activity occurs in an asynchronous fashion over the two hemispheres and is usually accompanied by irregular respiration and irregular eye movements. The discontinuous EEG pattern is often referred to as tracé discontinu. Irregular respiration and occasional eye movements accompany tracé discontinu sleep. The terms indeterminate sleep and transitional sleep are used to describe periods of sleep that cannot be classified as either quiet or active sleep.
Between 27 and 30 weeks CA, the EEG is usually discontinuous and the background activity is asynchronous. With increasing age, the periods between bursts become increasingly shorter. Central and temporal sharp wave transients are common features during this age. Posterior predominant delta waves with superimposed 14- to 24-Hz activity called delta brushes appear. During quiet sleep, the EEG is discontinuous and eye movements are rare. During active sleep, continuous delta or theta-delta activity predominates. Cardiac and respiratory rhythms are more regular and apparent during quiet sleep than during active sleep.
Between 30 and 33 weeks CA, there is discontinuous activity with occipital delta activity. A low-voltage, mixedfrequency, and nearly continuous EEG pattern occurs during active sleep. However, during quiet sleep, the EEG remains discontinuous, and bursts of high-voltage delta activity followed by 10 seconds of low-voltage activity can be observed. Temporal and frontal sharp transients and delta brushes remain the prominent EEG patterns. With the emergence of distinctive active and quiet sleep patterns, transitional sleep also becomes more prominent at 32 to 33 weeks CA (2). At 34 weeks CA, nonrapid eye movement (NREM)—REM cycle duration is approximately 45 minutes, which increases to 60 minutes at 38 weeks CA or full-term infant.
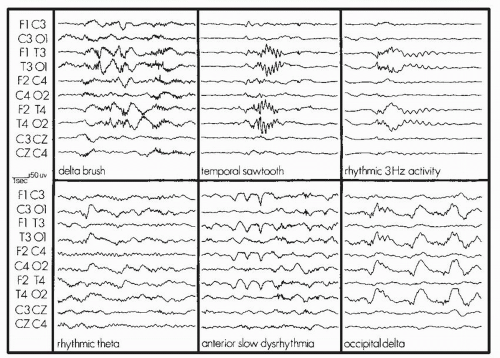
At 33 to 35 weeks CA, continuous predominantly slow activity (1-2 Hz) occurs during wakefulness. Delta brushes are prominent, especially in the occipital and rolandic regions. Multifocal sharp transients and anterior slow dysrhythmia, a frontal mono or polymorphic, >0.5-Hz, delta activity, are also common normal findings in the premature infant. Anterior slow dysrhythmia slower than 0.5 Hz in the premature neonate is associated with a poor outcome. There is discontinuous activity in quiet sleep. Active sleep has a continuous pattern similar to that of wakefulness. At 33 to 34 weeks CA, muscle tone decreases during active sleep relative to quiet sleep (3).
Between 33 and 37 weeks CA, features including smiling, grimaces, and body twitches are present during active sleep. By 37 weeks CA, active sleep is well differentiated. Medium-voltage and continuous EEG, REMs, irregular breathing patterns, muscle atonia, and phasic twitches of the face and extremities are present. During quiet sleep, breathing patterns are regular and body movements are rare. The EEG during quiet sleep shows an alternating pattern (tracé alternant [TA]) in which 1- to 10-second bursts of moderate- to high-amplitude delta activity alternate with 5- to 10-second intervals of lowvoltage mixed-frequency theta activity. Beginning at approximately 37 weeks CA, the EEG becomes more continuous with increasing age.
TABLE 2-1 EEG PATTERNS USED IN INFANT SLEEP STAGING
EEG PATTERN
LVI
Low voltage (14-35 µV), little variation Theta (5-8 Hz) predominates Slow activity (1-5 Hz) also present
TA
Bursts of HVS waves (1-3 Hz) with superimposed rapid low-voltage sharp waves (2-4 Hz) alternating with low-voltage mixed-frequency activity lasting for 4-8 seconds
Beginning at approximately 38 weeks CA, activité Moyenne, a continuous 1 to 10 Hz but predominantly 4 to 7 Hz, 25 to 50 µV background becomes the primary activity during wakefulness and active sleep.
The normal patterns recorded from various CAs are shown in Figures 2-1, 2-2, 2-3.
TABLE 2-2 CHARACTERISTICS OF WAKEFULNESS, ACTIVE SLEEP, AND QUIET SLEEP
WAKE
ACTIVE SLEEP
QUIET SLEEP
INDETERMINATE
Behavioral
Eyes open Frequent movement
Eyes closed Facial movements: smiles, grimaces, frowns Burst of sucking Body—small digit or limb movements
Eyes closed No body movements except startles and phasic jerks Sucking may occur
Not meeting criteria for active or quiet sleep
EEG
LVI, M
LVI, M, HVS (rarely)
HVS, TA, M
Electrooculography (EOG)
REMs Saccades
REMs A few slow eye movements (SEMs) and a few dysconjugate movements may occur
No REMs
EMG
High, variable
Low
High
Respiration
Irregular
Irregular
Regular Postsigh pauses may occur
DEVELOPMENT OF SLEEP-WAKE CYCLE
Infancy
Newborn term infants do not have the well-developed adult EEG patterns to allow staging according to Rechtschaffen and Kales rules. Infant sleep is divided into active sleep (corresponding to REM sleep), quiet sleep (corresponding to NREM sleep), and indeterminate sleep, which is often a transitional sleep stage. Behavioral observations are critical. Wakefulness is characterized by crying, quiet with eyes open, and feeding. Sleep is often defined as sustained eye closure. Newborn infants typically have periods of sleep lasting 3 to 4 hours, interrupted by feeding, and total sleep in 24 hours is usually 16 to 18 hours. They have cycles of sleep with a 45- to 60-minute periodicity with about 50% active sleep. In newborns, the presence of REM (active sleep) at sleep onset is the norm. In contrast, the adult sleep cycle is 90 to 100 minutes, REM occupies about 20% of sleep, and NREM sleep is noted at sleep onset.
The EEG patterns of newborn infants have been characterized as low-voltage irregular (LVI), TA, HVS, and mixed (M). Eye movement monitoring is used as in adults. An epoch is considered to have high or low electromyography (EMG) if more than one-half of the epoch shows the pattern. The change from active to quiet sleep is more likely to manifest indeterminate sleep. Nonnutritive sucking commonly continues into sleep.
Note that the sleep of premature infants is some-what different from that of term infants (36-40 weeks’ gestation). In premature infants, quiet sleep usually shows a pattern of tracé discontinu. This differs from TA as there is electrical quiescence (rather than a reduction in amplitude) between bursts of high-voltage activity. In addition, delta brushes (fast waves of 10—20 Hz) are superimposed on the delta waves. As the infant matures, delta brushes disappear and TA pattern replaces tracé discontinu.
FIGURE 2-1 Normal patterns recorded in subjects at the following CAs (left to right and above to below): 33, 30, 29, 35, and 28 weeks. (From Stockard-Pope JE, Werner SS, Bickford RG, eds. Atlas of neonatal electroencephalography. 2nd ed. New York: Raven Press, 1992, with permission.)
The term infant spends about one-third of the time in the awake state. The remaining two-thirds (˜16 hours) of time is equally divided between NREM and REM sleep. Sleep-wake states alternate in 3- to 4-hour cycles, with randomly timed phases of wakefulness, active sleep, and quiet sleep. Within the first month following birth, sleep-wake phase organization begins to adapt to the light-dark cycle and to associated social cues. The circadian rhythm of temperature appears first. Soon after birth, circadian wake rhythm then appears (˜day 45 of life). Circadian sleep rhythm appears around day 56 of life (4). By 10 to 12 weeks of age, the development of neural systems produces a steady diurnal distribution of sleep and wake.
During the first 3 months of life, infants spend 50% of their sleep time in REM (active sleep) and 50% in NREM (quiet sleep). The proportion of sleep in REM and NREM changes dramatically during the first year of life. Sleep time declines to 13 hours at 1 year of life. REM sleep declines from 7 to 8 hours at birth to 6 hours by 6 months of life and then to 4 to 5 hours by 1 year of life. During the first month of life, sleep-onset REM occurs two-thirds of the time, declining to 20% by 6 months of life (2,5). With a steady decline in the proportion of REM sleep, NREM sleep becomes more predominant during the first half of the sleep cycle, and REM sleep predominates during the latter half of the sleep cycle. The latency before entering REM sleep gradually increases during the first year. The REM-NREM cycle length is between 60 and 70 minutes during the first year of life. By 4 to 5 years of age, the cycle length gradually increases to 90 minutes. By 10 years of life, total REM sleep resembles adult proportions of approximately 20% to 25% of total sleep time (TST), with the child averaging 9 hours of total sleep in a single nocturnal sleep period (6).
The appearances of specific waveforms in the EEG represent a significant milestone in sleep ontogeny. Sleep spindles begin to appear at 4 weeks of age, rapidly develop through 8 weeks of age, and characterize NREM sleep by 3 months (7). Sleep spindles increase in number by 6 months of age, although there is often inter-hemispheric asynchrony of spindles until the age of 2 years (8). K complexes are detectable on the EEG by 3 months and are fully developed by 2 years of age (9). High-voltage, low-frequency theta (4-8 Hz) or delta (0.5-4 Hz) waves are detectable, particularly over the occipital area, at around 1 month of age. The three stages of NREM sleep are distinguishable electrophysiologically by 6 to 12 months of age. The circadian rhythm in a child’s sleep patterns, detectable by 3 to 6 months, gradually comes under the control of external stimuli, including light exposure. It is common by 6 months of life to sleep throughout the night, with the appearance of a predominantly biphasic pattern, with an afternoon nap. The cycles of REM sleep develop by 3 months.
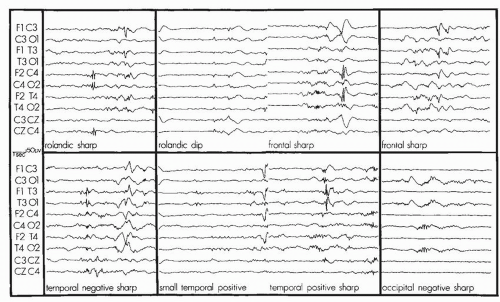
FIGURE 2-2 Series of EEGs illustrating variability in location, amplitude, and duration of transients recorded in low-risk premature infants at the following CAs (left to right and above to below): 30 weeks, 28 weeks, 28 weeks, 33 weeks, 30 weeks, 33 weeks, and 30 weeks. (From Stockard-Pope JE, Werner SS, Bickford RG, eds. Atlas of neonatal electroencephalography. 2nd ed. New York: Raven Press, 1992, with permission.)
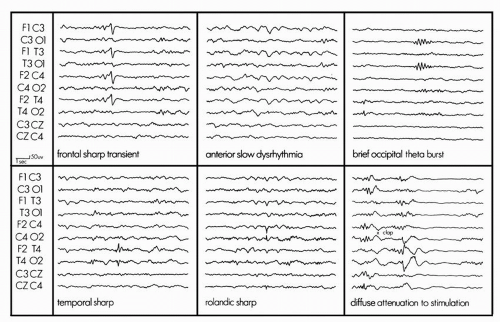
FIGURE 2-3 Common patterns and transients seen in the term newborn. (From Stockard-Pope JE, Werner SS, Bickford RG, eds. Atlas of neonatal electroencephalography. 2nd edn. New York: Raven Press, 1992, with permission.)
Childhood
The posteriorly dominant “alpha rhythm” is first seen at approximately 6 months of life but is slow. The frequency of the posteriorly dominant rhythm typically increases to 8 Hz by 3 years of life. Some individuals may lack an obvious posteriorly dominant rhythm as a normal variant.
As children progress through the first decade of life, adult patterns begin to emerge. During the first year of life, TST gradually decreases and, by 2 years of age, sleep occupies around 11 hours at night and up to 2.5 hours of sleep during one or two daytime naps. Thirty percent of a child’s sleep is REM sleep. Total daily sleep continues to decrease, but at a progressively slower rate during childhood. The afternoon nap is often retained until the age of 5 years. During childhood, sleep latency is shorter than in later life, averaging 5 to 10 minutes. Sleep efficiency is approximately 95%, and the percentage of stage 3 NREM sleep is greater than at any other age. Body movements during sleep begin to decrease in frequency, although they are more often seen in middle childhood than in adolescents or young adults (4). Between 5 and 10 years of age, sleep architecture matures to an adult-like pattern, with slow-wave sleep occurring during the first one-third to one-half of the nocturnal sleep time and REM sleep increasing in volume and intensity as the night progresses (4). Stage 4 NREM sleep decreases from 18% in 6- to 7-year-olds, to 14% in 11-year-old children. This decline in stage 4 NREM sleep is associated with an increase in stage 2 NREM sleep. Other NREM sleep stage proportions remain the same. REM latency decreases from 140 minutes in 6- to 7-year-olds to 124 minutes in 10- to 11-year-old children. The number of REM periods and amount of activity during REM also decreases with increasing age (1,10). TST decreases to around 9 hours daily, as seen in adults.
Only gold members can continue reading. Log In or Register to continue