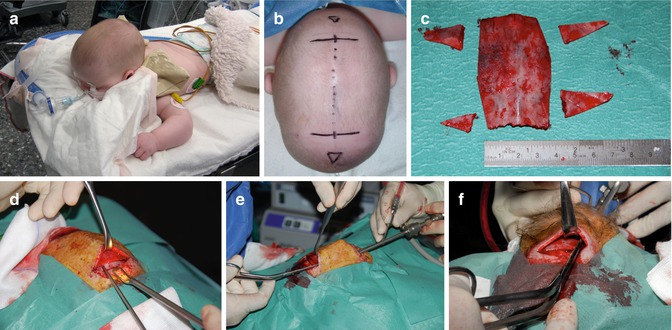
Fig. 17.1
Extent of suturectomy in (a) scaphocephaly, (b) trigonocephaly, and (c) frontal plagiocephaly
To perform endoscopy and thus claim a “minimally invasive technique” is not a goal in itself. The use of the endoscope must be regarded as an additional tool that improves illumination and visibility, thus allowing small skin incisions without compromising optical control. The endoscope is used for dural dissection and relieving the dura from the bone and synostotic suture. This is usually easily done, since dura is hardly attached to a synostotic suture, which is in strong contrast to dura that is firmly attached to intact cranial sutures. The endoscopic control allows early optical control of emissary veins that then can be coagulated and cut.
EACS should be considered simple and easy surgery if it is well performed.
17.2.1 Diagnostics
Craniosynostosis requires neurological, ophthalmological, radiological, and human genetics diagnostic evaluation, but these are nonspecific and independent of the type of surgery chosen. A skull X-ray does not contribute to the diagnostics, but we consider a 3D CT scan of the skull obligatory. Not as much as to establish a diagnosis, since the diagnosis can be obtained by simply observing and investigating the patient, but to acquire as much information as possible to be optimally prepared for surgery. Attention should be paid to opacities in the bone that can be present in the small baby so that inadvertent breaking or perforating of the skull can be prevented. Sometimes the affected suture is not completely synostotic. The open part of an otherwise synostotic suture does not necessarily have to be removed. Also, since the dura is more firmly attached to the open suture as compared to the synostotic suture, this should be known to prevent the risk of dural laceration. The thickness of the skull that can be irregular should be addressed also, as usually a pair of scissors is used to cut the skull under endoscopic view. The skin incision should be determined paying attention to all these factors.
For evaluation of the surgical result, we do not want to rely on radiological examinations because of the irradiation. Therefore, we prefer 3D stereophotogrammetry in the preoperative setting that can be repeated unrestrictedly during many years of follow-up.
17.2.2 Timing of Surgery
Jimenez and Barone already found that the critical age for EACS seems to be 6 months. After that age the cosmetic results become worse, and insufficient correction of skull shape is reached. However, one should not wait until the infant reaches the age of 5 or 6 months. The earlier an EACS is performed, the better the result. This is of even more importance in case of plagiocephaly and trigonocephaly. Therefore, below the age of 4 months, we always offer EACS as the treatment of choice, but, for infants of 5 or 6 months, we restrict EACS for mild and moderate cases and consider open remodeling procedures for severe cases. An optimal age for EACS is in our opinion 3 months. The child has grown after birth and acquired some weight, can tolerate some moderate blood loss, and is able to tolerate the molding helmet. Unfortunately, there is quite often a significant diagnostic delay with general practitioners and pediatricians, because of which many patients are seen in a later phase and this goal of surgery at 3 months cannot be reached.
In syndromic cases diagnosis is usually obtained early after birth. This offers a window of opportunity for early treatment. We prefer to operate these children at an age of 4–8 weeks. The idea is not to offer a definitive treatment of for instance the brachycephaly but to reduce a progressive deformity and prevent increased intracranial pressure. Parents are informed that cranial vault expansion and bifrontoorbital advancement procedures may still be required at a later stage. Because of the very young age and additional problems, such as sleep apnea, redression helmet therapy is not added in these cases. At this moment, however, the experience in syndromic cases of craniosynostosis is evolving, which may change our policy in the future.
17.2.3 Anesthesia, Monitoring, and Postoperative Care
Standard anesthetic monitoring techniques are used, including electrocardiography, noninvasive blood pressure monitoring, pulse oximetry, temperature monitoring, and blood loss monitoring. EACS on the metopic and coronal sutures is performed with the patient in a supine position. The sagittal suture is best operated upon with the patient in a sphinx position (see Fig. 17.4a), while the lambdoid sutures are reached with the patient in a prone position.
Since blood loss is usually minimal and OR times limited to 45–75 min, a central venous line is not required nor an arterial line. Two peripheral venous lines suffice in all cases. Antibiotic prophylaxis consists of 25 mg/kg cefazolin i.v. given 20 min before skin incision in all cases. All patients are monitored postoperatively in pediatric high dependency unit, and hemoglobin/hematocrit is controlled at the end of surgery and 6 h later. ICU monitoring is never needed. Postoperative pain is treated with prophylactic paracetamol and low-dose i.v. morphine until the first day after surgery. The patient is usually dismissed from the hospital on the first or second postoperative day.
In our series postoperative blood transfusion was required in 15 % of cases, while intraoperative blood transfusion was never required. The only postoperative complication was a Norovirus infection in one case. We have not encountered infection, air embolus, hyponatremia, hypotension, injury to the sagittal sinus, dural tear, postoperative hematoma, seizure, coagulopathies, or mortality in 40 successive cases of EACS.
17.2.4 Instrumentation and Surgical Hemostasis
EACS can be performed with a standard armamentarium. To limit blood loss, we use monopolar cutting for galea and periosteum. The endoscope is a Storz 0° lens scope with a working shaft used for endoscopic facial lift surgery without irrigation or suction (Fig. 17.2). A separate aspirator parallel to the endoscope performs blood aspiration. Craniectomy is performed with a high-speed drill initially and continued with different rongeurs and Kerrisons. In scaphocephaly, a pair of strong scissors is used to cut the bone from one craniectomy site to the other in order to remove a piece of bone of 11 × 4 cm (see Fig. 17.4c, f).

Fig. 17.2
Endoscope, endoscope shaft, and instruments used in EACS
Bleeding during surgery from the epidural space and bone edges is easily controlled with FloSeal® Matrix Hemostatic Sealant (Baxter Healthcare Corporation, Fremont, CA, USA).
17.2.5 Helmet Molding Therapy
Within 2 weeks after surgery, a plaster imprint of the skull is taken, which serves as an initial template for the fabrication of the custom-made helmet.
The children are wearing the helmet within 3 weeks postoperatively. During follow-up special attention is paid concerning the development of pressure ulceration areas and/or other complications due to the wear of the helmet.
Changes in cranial shape occur immediately after initiation of the surgery and are noted especially postoperatively. The helmet corrects the calvarial growth pattern and, subsequently, the direction of growth. The plasticity of the infant cranial vault, along with rapid brain growth during the first months of life, permits skull remodeling in the postoperative time. Whereas, our data also confirmed that after approximately 6 months, the helmet is used to maintain the cephalic index and prevent or reduce a relapse of the deformity [13].
There are different types of molding helmets on the market for positional occipital plagiocephaly. However, they may not all be suitable for treatment of craniosynostosis. We experienced an improvement of our results, especially in case of scaphocephaly, after we changed from a one-piece helmet to a two-piece helmet (Fig. 17.3). The advantage of the two-piece helmet is that these are thinner and lighter, better aerated, easier to put on and off, more stable on the head (less “sliding” of the helmet), and easily adjustable shaping by heating the helmet.

Fig. 17.3
Two-piece molding helmet
In our series the helmet is worn for 10 months (range 6–16 months) on average. None of the patients developed pressure ulcer, whereas dry skin or development of eczema under the helmet was documented in two patients. These dermal problems were resolved after finishing the helmet therapy.
17.3 Scaphocephaly
Scaphocephalic patients are positioned in a modified prone sphinx position bringing the synostotic sagittal suture in a horizontal plane (Fig. 17.4). The craniectomy is performed from the anterior to the posterior fontanelle but may be adapted in case a part of the suture is still open and patent. The removed strip should be 4–5 cm wide. Lateral barrel stave osteotomies or wedge-shaped osteotomies behind the coronal sutures and in front of the lambdoid sutures should assist in allowing an increased biparietal width (Fig. 17.4c). A video demonstrating this surgery can be seen on http://www.youtube.com/watch?v=oUIEhPsKT3E.
 Current Status and Future Developments of Neuroendoscopic Management of Pituitary Tumours and Craniopharyngiomas
Current Status and Future Developments of Neuroendoscopic Management of Pituitary Tumours and Craniopharyngiomas
 Neuroendoscopy in Spinal Pathology: Our Experience, New Trends, and Developments
Neuroendoscopy in Spinal Pathology: Our Experience, New Trends, and Developments
 Endoscopic Treatment of Hypothalamic Hamartomas
Endoscopic Treatment of Hypothalamic Hamartomas
 Neuroendoscopic Treatment of Colloid Cysts
Neuroendoscopic Treatment of Colloid Cysts
 The Application of Neuroendoscopic Techniques in Improving Altered CSF Physiology
The Application of Neuroendoscopic Techniques in Improving Altered CSF Physiology
 Neuroendoscopic Management of Intraparenchymal Lesions
Neuroendoscopic Management of Intraparenchymal Lesions




Related posts:
Current Status and Future Developments of Neuroendoscopic Management of Pituitary Tumours and Craniopharyngiomas
Neuroendoscopy in Spinal Pathology: Our Experience, New Trends, and Developments
Endoscopic Treatment of Hypothalamic Hamartomas
Neuroendoscopic Treatment of Colloid Cysts
The Application of Neuroendoscopic Techniques in Improving Altered CSF Physiology
Neuroendoscopic Management of Intraparenchymal Lesions
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
