Endovascular Treatment of Ischemic Stroke
Key Points
Techniques for endovascular revascularization of acute ischemic stroke are capable of achieving consistent success rates of over 90%.
Angiographic revascularization of ischemic stroke has become conflated with clinical efficacy. These are two entirely separate, and often unrelated, phenomena.
More than 80% of strokes worldwide are ischemic in origin and one in five of these affect the posterior circulation. Ischemic stroke is a heterogeneous diagnostic categorization involving a multitude of variables including age, cardiovascular health status, location and nature of the ischemic lesion, and the physiologic impact of the lesion in each individual patient. Identifying a single treatment modality that can improve outcomes in the setting of so many diverse circumstances has been and continues to be difficult.
Intravenous Thrombolysis
Intravenous thrombolysis for acute ischemic stroke was described as far back as the 1950s (1). However, the first trials of intravenous thrombolytic agents administered within 6 hours of onset of ischemic stroke were not auspicious. Hemorrhage rates were unacceptably high with intravenous streptokinase, and a defined therapeutic impact was not evident with early trials of tPA probably due to the late timing of treatment (2,3,4). Finally, in 1995 with publication of the NINDS rt-PA study FDA approval was gained for use of intravenous recombinant tissue plasminogen activator (rt-PA) within 3 hours of onset of symptoms (5). A modest improvement in 90-day outcome was seen in patients treated with rt-PA compared with placebo. Patients treated with tPA were 30% more likely to have a good outcome at 90 days compared with patients treated with placebo. Symptomatic hemorrhage within 36 hours of administration of tPA was seen in 6.4% of tPA patients, while mortality rates in the tPA and placebo groups were similar at 17% and 21%, respectively. In 2008 the ECASS-III study additionally demonstrated a small but statistically significant effect of intravenous rt-PA in stroke patients during the 3- to 4.5-hour period since onset (6). Patients treated in this time window were 28% more likely to have a favorable outcome on the Modified Rankin Scale compared with placebo. Rates of symptomatic hemorrhage were higher with tPA (2.4% vs. 0.3%) and overall hemorrhage rates were substantially higher (27% vs. 17.6%) but without any difference in mortality rates (7.7% vs. 8.4%).
From trials of intravenous thrombolytic agents and other studies it was inferred that clinical improvement of the patient bore some relationship to the success of recanalization, although this correlation was difficult to define precisely. Independent of any thrombolytic agent, approximately 25% of all ischemic strokes will recanalize spontaneously within 24 hours and more than 50% will do so within 1 week (7,8,9). Administration of thrombolytic drugs improves acute recanalization rates to approximately 46% overall, and the chances of a good outcome at 3 months are increased by a factor of 4 or 5 in patients with immediate and sustained recanalization (7). Nevertheless, a good therapeutic outcome following intravenous thrombolytics is seen in substantially less than half of treated patients, and a sizeable proportion of patients deteriorate even in the absence of contraindications to administration of the drug (10).
In summary, intravenous thrombolytic therapy by itself helps at best only about a third of those ischemic stroke patients who are eligible for its strictly defined criteria, even when stretched to include presentation within 4.5 hours. Timing of administration is a factor, being twice as efficacious within the first 1.5 hours after onset of a stroke as it is when administered within 1.5 to 3 hours (6). Symptomatic intracranial hemorrhage occurs in 1.7% to 8% of treated patients (5,6,11), and many patients are ineligible for this treatment due to late presentation or other reasons.
Intra-Arterial Treatment of Ischemic Stroke
Due to the shortcomings and limitations of intravenous thrombolytic therapy for acute ischemic stroke the drive to develop intra-arterial techniques of recanalization has been strong since the method was first described (12,13). Intra-arterial therapy offers several theoretical and actual advantages compared with bedside drug administration including
the capacity to deliver higher concentrations of local fibrinolytic agents into the clot itself and to monitor the state of vessel recanalization angiographically (Fig. 32-1). Furthermore, there is the potential to use several different mechanical techniques and devices sequentially until a winning solution is achieved (Figs. 32-2 and 32-3). However, it must be emphasized that the overarching focus on arterial recanalization in the literature dealing with intra-arterial therapy as a biomarker for successful therapy is potentially misleading. Given the correct circumstances endovascular recanalization of an ischemic lesion can be helpful, but recanalization
is not synonymous with reversal of ischemia or with the assurance of a good outcome.
the capacity to deliver higher concentrations of local fibrinolytic agents into the clot itself and to monitor the state of vessel recanalization angiographically (Fig. 32-1). Furthermore, there is the potential to use several different mechanical techniques and devices sequentially until a winning solution is achieved (Figs. 32-2 and 32-3). However, it must be emphasized that the overarching focus on arterial recanalization in the literature dealing with intra-arterial therapy as a biomarker for successful therapy is potentially misleading. Given the correct circumstances endovascular recanalization of an ischemic lesion can be helpful, but recanalization
is not synonymous with reversal of ischemia or with the assurance of a good outcome.
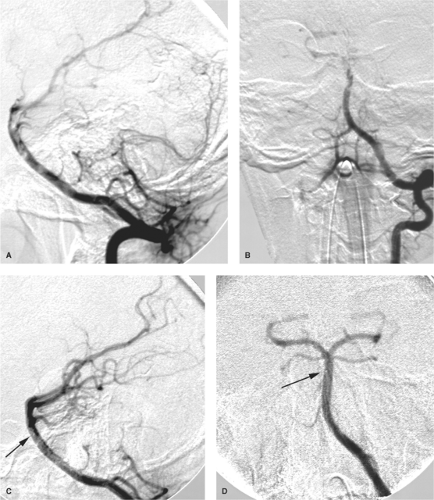 Figure 32-1. (A–D) Acute basilar artery thromboembolism during pregnancy. A young female who was 8 weeks pregnant presented following a long air flight with signs of posterior fossa ischemia. Her MRA demonstrated attenuation of flow signal in the basilar artery. She responded well to heparin at first but after approximately 18 hours became suddenly obtunded and hemiparetic. Left vertebral angiography, lateral (A) and PA (B) views, demonstrated an elongated filling defect in the upper two-thirds of the basilar artery with poor filling of the left posterior cerebral artery and superior cerebellar arteries. Thrombolysis was performed at various points within the thrombus through a microcatheter using a total of 600,000 units of urokinase. Lateral (C) and PA (D) views after urokinase show complete filling of the previously nonvisualized branches. The microcatheter tip is indicated with an arrow; the injection of contrast was made through the introducer catheter. The patient left the hospital with a residual deficit of a mild VI palsy. Her pregnancy was apparently unaffected, and she subsequently had an endovascular repair of a patent foramen ovale, which had been instrumental to the genesis of this paradoxical embolus. Pregnancy is mentioned as a contraindication to the use of urokinase, but under circumstances such as these, all contraindications are relative. |
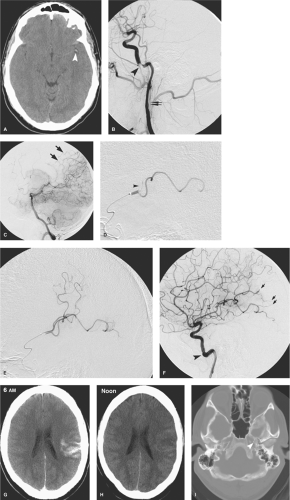 Figure 32-2. (A–I) Successful thrombolysis in the left middle cerebral artery outside of the 0- to 6-hour window, undoubtedly due to the large role played by the pial–pial collateral vessels. A young father of three children sustained a trivial sports injury to the neck at approximately 7 PM and soon thereafter developed a fluctuating aphasia and right-sided hemiparesis. Largely due to the insistence of his wife despite temporary spontaneous improvement, his discharge home from an outside hospital was countermanded, and he was transferred to our hospital by which time his condition had deteriorated again. His initial 1 A.M. CT (A) demonstrated no evidence of extensive ischemic injury in the left hemisphere, but the left middle cerebral artery trunk and bifurcation show a “dense MCA sign” (arrowhead). His left common carotid artery injection (B) shows an extensive dissection of the left internal carotid artery (double arrows) with a near-occlusive intimal sock (arrowhead) in the petrous section. The posterior division of the left middle cerebral artery is not filling. The superior division is filling well, implying that the embolus seen on the initial CT that caused his presenting aphasia has broken up and moved distally. A left vertebral artery injection taken later during the procedure (C) shows that the patient has some collateral flow (arrows in C) to the distal branches of the affected territory. In one of those instances of inexplicable good fortune, a microcatheter seemed to find its own way past the dissection to the main residual site of occlusion (D), where a saddle embolus (arrowhead in D) sits astride the bifurcation between the angular branch and the parietal branches. This responded very well to an infusion of 250,000 units of urokinase, following which the territorial perfusion was much improved (E). An attempt to stent the petrous carotid artery with a coronary stent precipitated a calamitous complete occlusion of the carotid artery, and for several minutes, the left hemisphere was dependent on collateral flow via the left ophthalmic artery. The situation was rescued by placement of a Neuroform stent in the artery (arrowhead in F). Distal microemboli are still evident in posterior hemisphere (small arrows in F), but this territory is rescued by the pial–pial collaterals from the posterior circulation in (C). His CT postprocedure at 6 A.M. (G) shows extensive patchy high attenuation in the left hemisphere, a finding easily confused for hemorrhage by those unfamiliar with this phenomenon. However, there is no mass effect associated with it and no fluid–fluid levels, and one can predict with reasonable confidence that the next CT (H) would demonstrate fading of this contrast staining that occurred in the territory of compromise of the blood–brain barrier. The bone windows (I) show that only the platinum tines (arrowhead) of the Neuroform stent can be discerned. A thrombolytic nihilist’s interpretation of these images would say that the patient was spontaneously improving anyway, that the embolus was breaking up and moving distally, and that the pial–pial collateral vessels were responsible for sustaining him during the period of occlusion, and that this case proves nothing. Certainly, the role of the collateral vessels is very important in a case such as this, but it is doubtful that they were sufficient to compensate completely for the occlusion. His clinical state of hemiparesis and aphasia were quite profound by the start of the procedure. Furthermore, it must be pointed out that the patient did make a very good recovery starting immediately after the procedure, considering that the affected territory involved his dominant hemisphere, and that this could not have been predicted to happen with IV thrombolytic from the NINDS data even if IV treatment had been started in the first 3 hours. It must also be allowed that the natural history of his near-occlusive dissection might not have been so good, considering that it had already induced cerebral thromboembolic complications once and might well have done so again without intervention. |
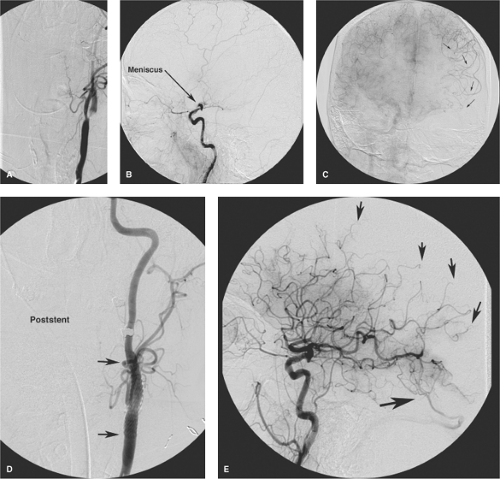 Figure 32-3. (A–E) Successful left carotid thrombolysis showing the importance of pial collateral flow, the illusion of a fixed “window” for all patients, and of preparedness to perform emergency carotid stenting. A middle-aged female was scheduled for elective head and neck surgery, for which her aspirin medication was discontinued. In the recovery unit after surgery at approximately 9 A.M., she developed a fluctuating neurologic deficit of aphasia and right-sided weakness. Between one thing and another, despite a progressive trend toward deterioration during the day, the first left common carotid arteriogram (A and B) was not performed until approximately 4.30 PM, by which time she was well outside the much touted 6-hour window for intervention. The AP view of the neck (A) and lateral view of the intracranial circulation (B) showed a critical stenosis of the left internal carotid artery origin with likely thrombus in the lumen and poor intracranial perfusion through this route. There is an apparent complete occlusion of the left middle cerebral artery with a meniscus sign (label in B). Most importantly, the right internal carotid artery (C) perfuses the left anterior cerebral artery territory from which several prominent pial–pial collateral pathways extend to reconstitute the left middle cerebral artery (arrows). An attempt was made at first to lyse the thrombus in the left middle cerebral artery by snaking a microcatheter through the stenosis and instilling tPA into the clot, but the effort was fruitless. Thinking that if we opened the carotid proximally we might be able to balloon angioplasty the clot in the left middle cerebral artery, we performed an angioplasty of the clotted stenosis and were surprised to see what an effect that had on the intracranial circulation. This site was then stented with the results shown on the left common carotid arteriogram (D) and lateral projection of the head (E). While some distal branches of the left middle cerebral artery show occlusions (small arrows), the overall appearance is dramatically different from that of a few minutes previously without addition of any more thrombolytic drug. Note the early venous opacification (larger arrow in E) indicating the likely establishment of infarction. The patient made a virtually complete recovery and was living a normal life within a month. The lessons from this case are manifold. First, what saved her was the fact that either through the effects of a long-standing stenosis or through some other mechanism, this patient had an unusual propensity to form pial–pial collateral channels to the affected territory. Second, the effect of a standard dose of thrombolytic drugs was miserable until flow was established by opening the stenosis proximally, a potential lesson for other situations where balloon angioplasty of clot might be considered. Third, her outstanding recovery in the time frame described underscores that the 6-hour rule does not apply to everybody. |
Three randomized trials of intra-arterial administration of thrombolytic drug for M1 or M2 occlusion have been published. The PROACT-II study identified a favorable outcome in 40% of patients treated with IA r-pro-UK versus 25% of placebo (heparin) patients, with a recanalization rate of 66% versus 18%, respectively (14). The Japanese MELT study also focused on MCA occlusions and found similar results (15). These studies were limited in scope and by the specific avoidance of mechanical disruption of the clot in the PROACT studies and only wire disruption in the MELT study, so the favorable outcome they describe is an indication of the power of even limited endovascular techniques in achieving recanalization. Since then, the expanding technologic capabilities of endovascular therapy have outraced and left behind the possibility of performing comprehensive randomized trials. Establishing vessel recanalization has become the de facto goal of treatment, with lesser attention paid to clinical outcome or complication rates, or so one might perceive from a review of the literature.
Endovascular intervention can achieve consistent rates of recanalization of 90% to 100% using a variety of snare, aspiration, balloon-angioplasty, and stent devices, particularly when multiple modalities are employed (16,17,18,19,20). These rates represent a considerable improvement over the recanalization rates seen with intravenous therapy alone (30% to 46%) and rates seen with exclusive use of intra-arterial thrombolytics or one mechanical device alone (60% to 70%) (21,22,23). Intra-arterial treatment of ischemic stroke can be performed on pediatric patients (24) and octogenarians sometimes with margins of safety and angiographic success comparable to those in other age groups, sometimes not (25,26), with only an occasional question being raised as to whether this is sustainable from a medical resource point of view, cost efficacy, or clinical outcome. The phenomenon of “futile recanalization” is well recognized and commonplace, that is, the acknowledgment that reopening an ischemic vessel really does not accomplish anything positive for the patient and may do a great deal of economic and medical harm. It is not uncommon for high double-digit published rates of futile recanalization (90%) or triple-digit rates of successful stent deployment to be juxtaposed with extremely modest rates of clinical improvement (27,28). The illusory success of achieving recanalization at such a high rate compounded with the phenomenon that aggressive stroke therapy is being touted as a showcase or marketing tool for many medical institutions means that the likelihood of rationalization or triage of stroke patients away from intra-arterial therapy seems even more improbable.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


