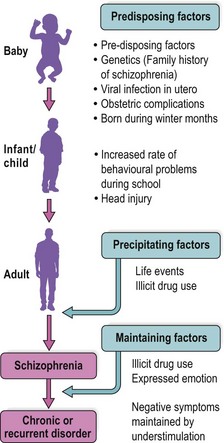
Epidemiology and aetiology of schizophrenia Much is known about the aetiology of schizophrenia but the exact nature of the condition is still unclear. One problem in researching this area is that schizophrenia is defined on the basis of symptoms for which there are no biological markers and there may be more than one underlying disease process. This possibility should be kept in mind when reading this section, in which the epidemiology of schizophrenia will be described, followed by a discussion of factors thought to be of aetiological importance. Epidemiology A striking finding of epidemiological surveys of schizophrenia is the similarity of prevalence in different countries. Most studies have found the lifetime prevalence of schizophrenia to be 7–9 per 1000 members of the population and, at any one time, 2–5 per 1000 population will have schizophrenia. There is not a great difference between these lifetime and point prevalence figures, which reflects the fact that schizophrenia is often a chronic illness. Men and women are affected equally. However, the average age of onset in men is usually late teens and twenties, whereas for women it is usually about 10 years later. Although the prevalence of schizophrenia is similar in different countries, some studies have found an altered risk in different parts of the world. Some of these variations are probably the result of studies using different diagnostic criteria. They may also reflect selective migration of people with schizophrenia. For instance, the high prevalence found in Northern Sweden may indicate that people with schizophrenia are more likely than others to tolerate life in an isolated community. Selective migration may also explain the high rates of schizophrenia found in some immigrant groups. An exception to this is the raised rate found in men of Afro-Caribbean origin in the UK, which is most apparent not in those who migrated but in their children. One explanation for this finding is that young black men are more likely to be misdiagnosed with schizophrenia because of cultural differences, and are more likely to be admitted to hospital, which may give a false impression of true prevalence rates. People with schizophrenia are more likely to be of lower social class than other members of the population. This is largely accounted for by social drift, a term used to describe the way people with schizophrenia drift down the social scale because of the effects of the illness. This phenomenon was demonstrated in a famous study which found that although people with schizophrenia were, on average, of lower social class, the social class of their fathers was representative of the general population. However, the social drift hypothesis may not be the only explanation. Some studies have shown that people with schizophrenia are more likely to have been born into deprived inner city areas. One explanation of this finding is that such environments may increase exposure to some of the risk factors for schizophrenia described later in this section. Aetiology The aetiology of schizophrenia is summarised in Figure 1. Fig. 1 The aetiology of schizophrenia. Genetics The finding that schizophrenia has a similar prevalence in different countries suggests that there is a large genetic component to its aetiology. This is supported by family studies which show that 8% of siblings and 12% of children of people with schizophrenia will also develop the condition. Twin and adoption studies suggest that this familial pattern is the result of genetic factors rather than shared environment. Monozygotic twins show a concordance rate for schizophrenia of 50% whereas for dizygotic twins the rate is only 20%. Adoption studies show a raised risk in biological but not adoptive relatives. A number of genetic variations have been found to be associated with schizophrenia. Most of these variations are common in the general population, and are responsible for only a small increase in risk. It is thought that when a number of these genetic variations occur together, and particularly in the presence of environmental risk factors, an individual’s risk of developing schizophrenia rises significantly.< div class='tao-gold-member'> Only gold members can continue reading. Log In or Register to continue Share this:Click to share on Twitter (Opens in new window)Click to share on Facebook (Opens in new window) Related Related posts: Mood stabilisers and ECT Old age psychiatry I Depressive disorder – clinical presentation Personality disorders – management Antipsychotic drugs Personality disorders – introduction and classification Stay updated, free articles. Join our Telegram channel Join Tags: Psychiatry An Illustrated Colour Text Jul 12, 2016 | Posted by admin in PSYCHIATRY | Comments Off on Epidemiology and aetiology of schizophrenia Full access? Get Clinical Tree
Epidemiology and aetiology of schizophrenia Much is known about the aetiology of schizophrenia but the exact nature of the condition is still unclear. One problem in researching this area is that schizophrenia is defined on the basis of symptoms for which there are no biological markers and there may be more than one underlying disease process. This possibility should be kept in mind when reading this section, in which the epidemiology of schizophrenia will be described, followed by a discussion of factors thought to be of aetiological importance. Epidemiology A striking finding of epidemiological surveys of schizophrenia is the similarity of prevalence in different countries. Most studies have found the lifetime prevalence of schizophrenia to be 7–9 per 1000 members of the population and, at any one time, 2–5 per 1000 population will have schizophrenia. There is not a great difference between these lifetime and point prevalence figures, which reflects the fact that schizophrenia is often a chronic illness. Men and women are affected equally. However, the average age of onset in men is usually late teens and twenties, whereas for women it is usually about 10 years later. Although the prevalence of schizophrenia is similar in different countries, some studies have found an altered risk in different parts of the world. Some of these variations are probably the result of studies using different diagnostic criteria. They may also reflect selective migration of people with schizophrenia. For instance, the high prevalence found in Northern Sweden may indicate that people with schizophrenia are more likely than others to tolerate life in an isolated community. Selective migration may also explain the high rates of schizophrenia found in some immigrant groups. An exception to this is the raised rate found in men of Afro-Caribbean origin in the UK, which is most apparent not in those who migrated but in their children. One explanation for this finding is that young black men are more likely to be misdiagnosed with schizophrenia because of cultural differences, and are more likely to be admitted to hospital, which may give a false impression of true prevalence rates. People with schizophrenia are more likely to be of lower social class than other members of the population. This is largely accounted for by social drift, a term used to describe the way people with schizophrenia drift down the social scale because of the effects of the illness. This phenomenon was demonstrated in a famous study which found that although people with schizophrenia were, on average, of lower social class, the social class of their fathers was representative of the general population. However, the social drift hypothesis may not be the only explanation. Some studies have shown that people with schizophrenia are more likely to have been born into deprived inner city areas. One explanation of this finding is that such environments may increase exposure to some of the risk factors for schizophrenia described later in this section. Aetiology The aetiology of schizophrenia is summarised in Figure 1. Fig. 1 The aetiology of schizophrenia. Genetics The finding that schizophrenia has a similar prevalence in different countries suggests that there is a large genetic component to its aetiology. This is supported by family studies which show that 8% of siblings and 12% of children of people with schizophrenia will also develop the condition. Twin and adoption studies suggest that this familial pattern is the result of genetic factors rather than shared environment. Monozygotic twins show a concordance rate for schizophrenia of 50% whereas for dizygotic twins the rate is only 20%. Adoption studies show a raised risk in biological but not adoptive relatives. A number of genetic variations have been found to be associated with schizophrenia. Most of these variations are common in the general population, and are responsible for only a small increase in risk. It is thought that when a number of these genetic variations occur together, and particularly in the presence of environmental risk factors, an individual’s risk of developing schizophrenia rises significantly.< div class='tao-gold-member'> Only gold members can continue reading. Log In or Register to continue Share this:Click to share on Twitter (Opens in new window)Click to share on Facebook (Opens in new window) Related Related posts: Mood stabilisers and ECT Old age psychiatry I Depressive disorder – clinical presentation Personality disorders – management Antipsychotic drugs Personality disorders – introduction and classification Stay updated, free articles. Join our Telegram channel Join Tags: Psychiatry An Illustrated Colour Text Jul 12, 2016 | Posted by admin in PSYCHIATRY | Comments Off on Epidemiology and aetiology of schizophrenia Full access? Get Clinical Tree