♦ Preoperative
Operative Planning
- Review imaging studies
- Non-contrast head computed tomography (CT) essential for precise localization of epidural hematoma (EDH) and for detecting skull fractures
- Consider dedicated maxillofacial CT for patient with severe trauma and multiple cranial/facial fractures that may need to be addressed simultaneously with EDH.
- Skull x-ray: most often does not add additional information to head CT
- Non-contrast head computed tomography (CT) essential for precise localization of epidural hematoma (EDH) and for detecting skull fractures
- Exploratory burr holes: With the prevalence of CT scanners, situations are increasingly rare in which a patient is deteriorating so rapidly that diagnostic studies are unobtainable and placement of exploratory burr holes is necessary.
- Surgical objectives
- Removal of clot: lowers intracranial pressure (ICP) and eliminates mass effect; clot is often thick so exposure of craniotomy should allow access to entire clot
- Hemostasis
- Prevention of hematoma reaccumulation with dural tenting
- Repair skull fracture, if necessary
- Removal of clot: lowers intracranial pressure (ICP) and eliminates mass effect; clot is often thick so exposure of craniotomy should allow access to entire clot
Equipment
- Mayfield head holder: clamp or horseshoe
- Basic craniotomy tray
- High-speed drill with appropriate drill bits
- Bone flap fixation tray
- Hemostatic agents (Avitene, Gelfoam, Surgicel, bone wax)
- ICP monitor or external ventricular drain system if needed
Operating Room Set-up
- Headlight and loupes
- Bovie electrocautery
- Bipolar cautery
Anesthetic Issues
- Preoperative intravenous antibiotics administered within 30 min prior to incision (cefazolin 2 g intravenously or clindamycin 600 mg intravenously)
- With underlying brain injury, consider loading with phenytoin (15 to 18 mg/kg) administered slowly, or alternatively, levetiracetam 1000 to 1500 mg intravenously
- Communicate with anesthesiologist suspected degree of ICP elevation and if needed:
- Hyperventilation to pCO2 of 30 to 35 mm Hg
- Mannitol 0.5 to 1 g/kg infusion starting at time of skin incision
- Propofol (if indicated)
- Surgeon should warn anesthesiologist of potential hypotension at the time of clot evacuation as blood pressure is often supported by a sympathetic response to increased ICP
- Hyperventilation to pCO2 of 30 to 35 mm Hg
♦ Intraoperative
Trauma Flap (Fig. 66.1)
- Position patient assuming cervical spine injury unless C-spine was cleared preoperatively.
- Bone flap should encompass margins of hematoma and be sufficient to repair skull fractures.
Technique
- Initial burr hole is made near the area of maximal clot thickness, often in the low temporal area, to allow for prompt decompression of the hematoma.
- Craniotomy that provides adequate access to hematoma margins is then completed.
- If bleeding is from the middle meningeal artery or its branches, bipolar cautery is usually sufficient.
- If bleeding is from the foramen spinosum, the foramen is plugged with bone wax.
- If bleeding is from the middle meningeal artery or its branches, bipolar cautery is usually sufficient.
- If the brain appears tight or there is a concern for underlying SDH, a small opening in the dura is made to inspect.
- Holes are drilled along the craniotomy margins for dural tenting sutures, ~2 cm apart. Several tenting sutures are also placed in the middle of the craniotomy bone flap.
Closure
- Wounds are irrigated copiously. Antibiotic containing irrigation can be used if concern for infection.
- Bone flap is replaced with several central tenting sutures to reduce volume of epidural space and at least three-point fixation with microplates and screws
- Repair skull fractures with additional microplates or mesh, if necessary
- Subgaleal drain may be placed to minimize postoperative collections
- Temporalis muscle and fascia is closed with 0–0 Vicryl interrupted sutures
- Inverted 0–0 and 3–0 Vicryl sutures are used to close the galea
- Staples to approximate the skin edges
- Xeroform and 4 × 4 dressings should be secured with a head wrap
< div class='tao-gold-member'>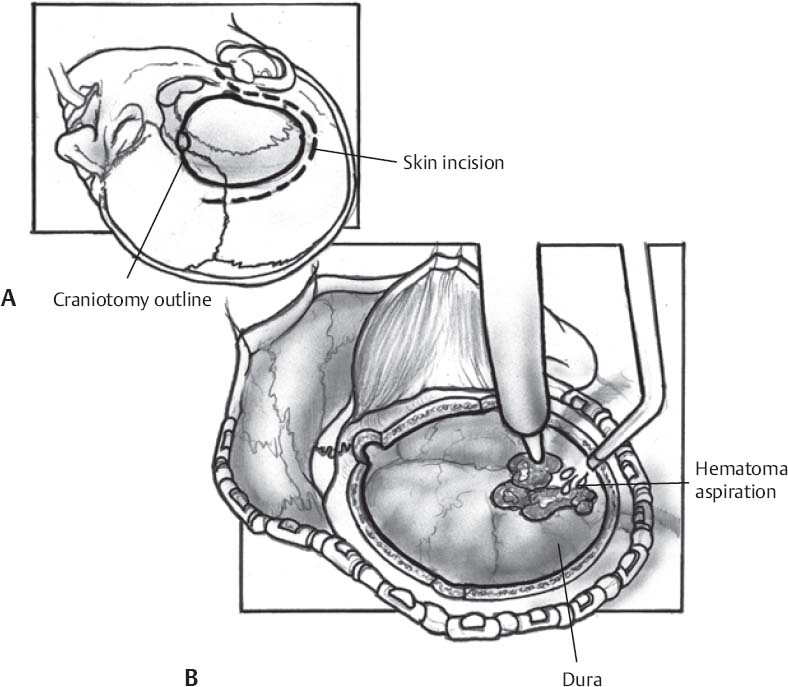 Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


