A presenting complaint of insomnia, whether a difficulty initiating sleep, maintaining sleep, or of inadequate sleep quality should lead to an evaluation pathway that is distinct from that for a complaint of excessive daytime sleepiness. The differential diagnosis for a complaint of insomnia is quite broad. Simply knowing that a person has insomnia is only the beginning of the evaluation. Most patients with insomnia report daytime fatigue as opposed to sleepiness.
THE PROMISE OF INSOMNIA ASSESSMENT (AND THE TIME COMMITMENT)
The numerous subtypes of insomnia provide an opportunity to make specific diagnoses and guide patients toward optimal treatment. Progress in our understanding of the causes of insomnia presents an opportunity for more effective treatment of insomnia, but success is dependent, primarily on adequate assessment.
Studies of clinical practice, however, suggest that insomnia most often goes unrecognized by the patient’s personal physician and in most instances it may not be assessed and treated. Surveys of general practice have found that physicians are often unaware of severe insomnia in their patients. Two studies found that 60% to 64% of cases went unrecognized (1,2). Even when physicians identify insomnia and medication is prescribed for sleep, there is usually no documented evaluation of sleep. In one study, 88% of the medical charts for patients receiving hypnotic medication contained no progress note reference to sleep (3).
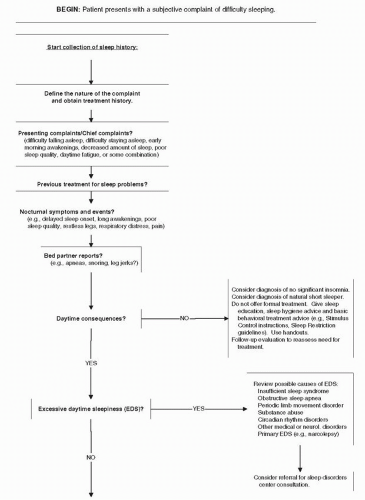
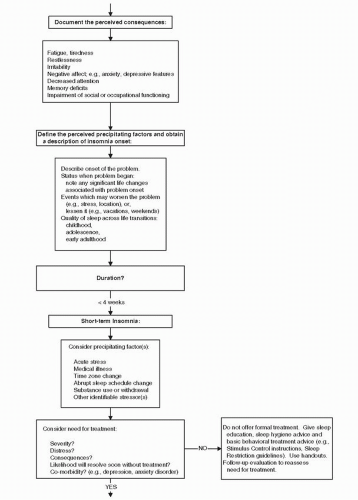
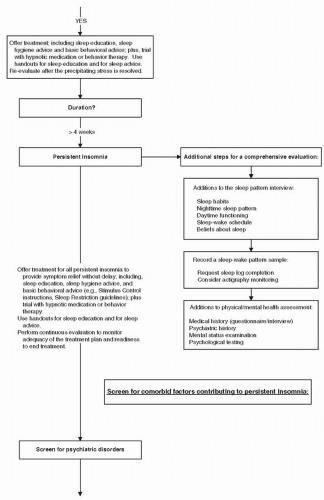
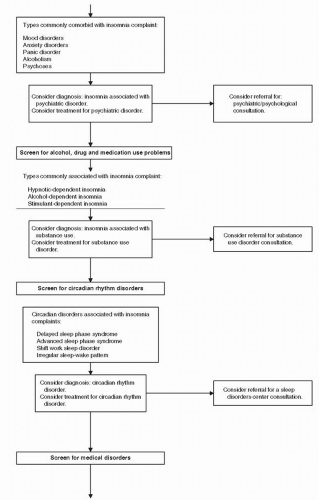
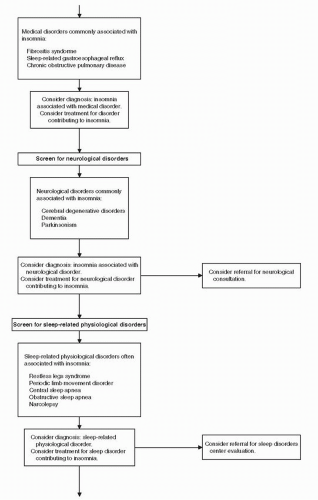
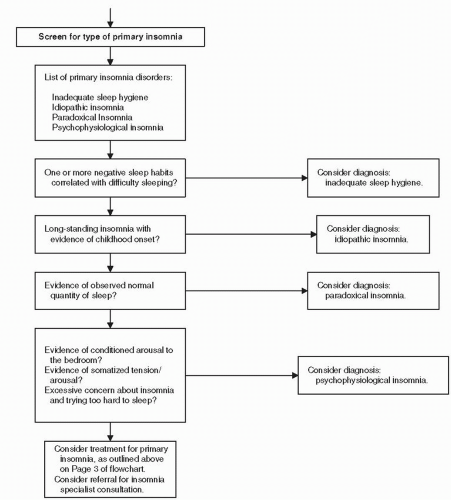
The large number of insomnia subtypes provides an opportunity for specificity in diagnosis and treatment; it also presents a potentially time-consuming assessment task. The following sections describe a structured assessment approach; the last section presents a diagnosis algorithm (Fig. 9-1); the structured approach is intended to facilitate time-efficient insomnia assessment.
INSOMNIA ASSESSMENT TOOLS
Sleep History (Begin with Reason for Referral)
Insomnia evaluation begins with history taking (see Tables 9-1, 9-2, 9-3 and 9-4). The information collection starts with reason for referral, specifically, history that focuses on (a) presenting complaints, (b) nocturnal symptoms, (c) bed partner reports, and (d) previous treatment of sleep problems.
It is also important to promptly elicit information about daytime consequences. The type of consequences can be an important indicator for etiology; for example, a history of excessive daytime sleepiness would suggest that the patient’s most primary problem is not insomnia. Patients with a primary insomnia disorder generally do not experience severe daytime sleepiness or fall asleep unintentionally during the daytime, because their basic problem is difficulty sleeping.
Chief Complaint
History taking begins with the patient’s description of sleep complaints. The chief complaint generally falls into one or more of the following categories: difficulty falling asleep, difficulty staying asleep, early morning awakenings, decreased total sleep time, poor quality sleep, or daytime fatigue.
Nocturnal Symptoms and Events
Some common symptoms of primary and comorbid insomnia disorders can be documented with patient report. These include increased arousal in the prebedtime period (suggesting conditioned arousal), restless legs symptoms, periodic leg movements (PLMs) (although this usually requires the observations of a bed partner), respiratory distress (including dyspnea, choking, and gasping), nocturnal panic attacks, pain, gastroesophageal reflux, and environmental noise. The report of these symptoms and events can help guide the initial sleep interview.
FIGURE 9-1 Algorithm for insomnia diagnosis and treatment selection.
FIGURE 9-1(continued).
FIGURE 9-1(continued).
FIGURE 9-1(continued).
FIGURE 9-1(continued).
FIGURE 9-1(continued).
TABLE 9-1 STANDARD SECTIONS OF A SLEEP HISTORY INTERVIEW
The primary sleep problem; including frequency, severity, duration, and perceived consequences
Previous treatment for sleep problems
Review of nighttime sleep: Presleep and sleep onset, sleep during the night, mornings
Daytime functioning
Sleep-wake rhythms
Sleeping environment
Beliefs about sleep
Development of the sleep problem, for example, onset of the problem, course, sleep across the lifespan
TABLE 9-2 INTERVIEW QUESTIONS FOR THE SLEEP HISTORY FOR INSOMNIA
What time do you get into bed at night?
Are you watching TV or reading at that time?
Do you fall asleep with the TV on?
If so, when do you turn it off?
How long does it take you to fall asleep once turn out the lights?
Do you sleep through the night or do you awaken?
How often do you awaken?
How long does it take you to return to sleep?
What do you do when awake at night?
Do you ever become angry or upset when awake in the middle of the night?
Do you look at the clock when you awaken during the night?
Do you ever have something to eat during the night?
What time do you get out of bed in the morning to start your day?
How long have you had this sleep pattern?
How much total sleep do you get per night?
How much sleep do you need to feel rested during the day?
What time did you go to bed and arise before you began to sleep poorly?
Bed Partner Reports
Bed partners (and anyone else who has observed the patient sleeping) are a potential source of information about nocturnal symptoms and the daytime consequences of insomnia. However, the validity of bed partner observations is limited by several factors. During the night, the bed partner will be sleeping and may have low awareness of the patient’s behavior. The bed partner can have subjective biases, for example, the loudness of snoring and the frequency of pauses in breathing or leg jerks during sleep may be exaggerated. Despite the inherent limitations, bed partners are sometimes the only good source of details about important nocturnal events including, limb movements during the patient’s sleep, snoring, and pauses in breathing during sleep.
Only gold members can continue reading. Log In or Register to continue