- Excessive daytime sleepiness (EDS) is a common symptom that is often overlooked despite causing significant disability in potentially all areas of daily activities
- Most commonly, EDS is secondary to conditions such as obstructive sleep apnoea which produce chronic insufficient or poor quality nocturnal sleep
- EDS may result from a primary sleep disorder in which there is proven or assumed cerebral pathology in brain areas involved in sleep regulation
- Narcolepsy is not rare and probably affects at least 1 in 3000 people
- Most narcoleptic subjects have a dysregulated sleep–wake cycle over 24 hours with particular abnormalities in the control of REM or dream sleep
- Full-blown narcolepsy is usually due to a specific neurochemical deficiency from the hypothalamus
- Focal or generalised muscle weakness when emotional suggests cataplexy, an extremely specific symptom that is virtually unique to narcolepsy
- Idiopathic hypersomnolence is a primary sleep disorder that may resemble narcolepsy but is less well characterised and generally less responsive to wake-promoting therapy
- Abnormalities of the internal clock (circadian misalignment) can cause significant EDS if due to extrinsic factors such as jet lag or shift work
- Increasingly, intrinsic abnormalities of circadian timing due to genetic variations are recognised
Introduction
Around 5% of the adult population experiences a level of daytime sleepiness that could be considered abnormal and potentially intrusive or even dangerous to routine daily activities. Complaints of drowsiness or an inappropriate and excessive tendency to nap during the day need to be carefully distinguished from simple ‘tiredness’, ‘fatigue’ or ‘lack of energy’. These phenomena usually have different aetiologies, such as chronic fatigue syndrome in which there is no objective evidence for an increased tendency to fall asleep.
When severe, excessive daytime sleepiness (EDS) should be treated as a potentially serious disability affecting most activities of daily living. Indeed, young subjects with EDS usually struggle to achieve their full potential, especially if untreated.
Unfortunately, EDS can still be dismissed by many as resulting merely from poor lifestyle habits, laziness or reduced motivation. In the past, EDS has even been considered as a ‘moral failing’. Consequently, the associated symptoms of poor concentration, motor clumsiness and automatic behaviours are frequently not recognised or, at best, misdiagnosed. Furthermore, EDS is often mistakenly attributed to reflect mood disorder (depression), hormonal balance (hypothyroidism) or anaemia, even though none of these typically produces EDS directly.
Formal diagnosis of a sleep disorder causing EDS may be delayed in youngsters who display behavioural problems of irritability or paradoxical hyperactivity rather than more obvious symptoms of sleepiness. Furthermore, teenagers and young adults, in particular, may seek to ‘self-medicate’ with recreational stimulant drugs. Potentially, this may also confuse or delay any underlying medical diagnosis and treatment.
The potential hazards of EDS when performing monotonous tasks such as driving are obvious and often preventable. Occupational health physicians are increasingly aware of EDS as an issue both at work and on the daily commute, especially in shift workers.
When caused by a sleep disorder, EDS is usually a persistent or chronic symptom although there are a few rare causes of intermittent sleepiness.
The term ‘hypersomnolence’ is virtually synonymous with EDS although strictly it refers to abnormally increased sleep time over the full 24-hour period. Importantly, some causes of EDS simply reflect sleepiness at unconventional times either because the sleep–wake cycle is dysregulated (e.g. narcolepsy) or because of abnormal circadian timing (e.g. jet lag). In these situations, total sleep time over the day–night cycle is usually of normal duration.
The physical signs of EDS are often subtle and may go unrecognised, particularly in the elderly, making a good history from the subject and close contacts particularly important. Slow eye blinking, yawning and brief spells of inattention (‘microsleeps’), even with eyes open, may be observable manifestations of EDS. Slurred speech, impaired fine motor control, resembling drunkenness and even personality change are apparent in severe cases.
Causes
The commonest cause of mild sleepiness is simply insufficient nocturnal sleep. Variably, this can reflect lifestyle choices, commitments through work or a poor quality sleeping environment. It can be surprising, however, how some subjects complaining of EDS do not appreciate the vital need for most to have around seven hours sleep at night, regarding it as a dispensable commodity. Such subjects typically report worsening EDS as the working week progresses and their ‘sleep debt’ mounts. Relative improvement in symptoms at weekends or on holiday with extended sleep periods would also be expected. It can occasionally be useful to obtain sleep diaries over a few weeks to demonstrate this pattern.
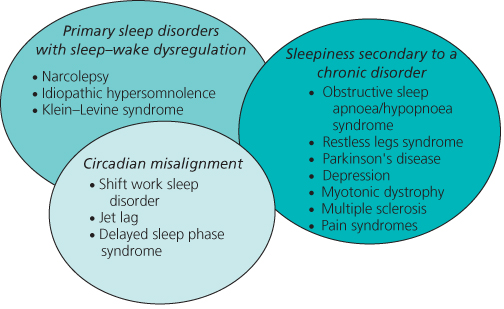
Aside from insufficient sleep, the causes of EDS can be broadly divided into three categories (Figure 3.1):
Figure 3.1 The causes of excessive daytime sleepiness (EDS) in patients seeking medical help may be divided into three main categories. Chronic disorders interfering with sleep quality form the biggest group by far. However, approximately 1 in 50 of subjects with EDS may have a primary sleep disorder such as narcolepsy. Circadian misalignment is an increasingly recognised cause of EDS. The categories are not mutually exclusive and may interact.
In practice, insufficient sleep due to work or social factors (e.g. noisy environment) is the commonest cause of mild EDS.
Narcolepsy
Narcolepsy has been recognised as a distinct syndrome for well over a century although it is only in the last decade that its underlying neurobiology has been established. Genetic analysis of a canine model of narcolepsy led to the surprising discovery that classical cases of human narcolepsy arise from specific destruction of a few thousand neurons in the lateral hypothalamus. This produces a deficiency of a neuropeptide called hypocretin (alternatively, orexin), a key regulator of the sleep–wake cycle. Although unproven, a variety of evidence suggests that the subtle neurological damage in narcolepsy has an autoimmune basis, occasionally with a defined precipitant such as a viral infection or vaccination.
Narcolepsy most frequently starts in early adolescence and is a life-long affliction. Given its specific neurochemical basis, it is perhaps not surprising that there is a spectrum of severity such that mild cases often escape medical attention. It probably affects as many as 1 in 3000 of Caucasian populations.
The most usual symptom of concern in narcolepsy is an inability to sustain useful alertness for more than about three hours. Irresistible sleep episodes, occasionally without recognising the prior imperative to sleep, may produce ‘sleep attacks’ in inappropriate situations and at any time of day. Naps are typically fairly short (around 20 minutes or less) and often refreshing. Many narcoleptics can sustain wakefulness if engaged in alerting activities but fight sleep if bored or unoccupied. Few can watch films without napping. Aside from frank sleep episodes, most will describe frequent so-called ‘microsleeps’ in which full awareness is diminished and automatic behaviours may occur with poor recall.
It is often not appreciated how badly narcoleptics sleep at night. Normal sleep architecture is generally disorganised, particularly during REM sleep periods which are fragmented and often intermixed with partial wakefulness. This produces vivid and often disturbing dreams at sleep–wake transitions, potentially confused with reality. Elements of REM sleep such as paralysis of voluntary muscles can also intrude into wakefulness, even at sleep onset. This symptom of sleep paralysis is not specific, however, and is commonly reported as an occasional disturbing phenomenon in normal populations.
The fragmented sleep of many narcoleptics almost certainly contributes to EDS and may merit specific drug therapy. Furthermore, virtually every parasomnia, including sleep walking and dream enactment (REM sleep behaviour disorder), can be seen more commonly in narcoleptics. In addition, other sleep disorders, notably obstructive sleep apnoea, may co-exist with narcolepsy and should not be overlooked, especially if symptom control appears to deteriorate with time.
By far the most specific and diagnostically important symptom in narcolepsy is cataplexy. This unusual phenomenon reflects the intrusion of REM sleep paralysis during wakefulness, most often when the subject is experiencing or expecting a positive emotion such as laughter or pleasant surprise. Attacks are generally brief and take a few seconds to build up, typically with head bobbing or facial jerking at the onset. This may suggest an epileptic phenomenon although a key feature of cataplexy is maintained awareness of the environment even when paralysed. Partial attacks are common and may be confined to slurred speech, transient neck flexion or sagging of the knees.
Rarely, cataplexy is the most troublesome symptom with numerous attacks each day, triggered by a range of emotions or situations. However, it is relatively rare for medical practitioners to witness cataplexy, as it usually occurs in relaxed circumstances with family or friends. It should be noted that over 30% of narcoleptics either have no symptoms of cataplexy or only very occasional episodes.
Investigations
Narcolepsy remains largely a clinical diagnosis based on a full history (Table 3.1). However, investigations may help to confirm clinical impressions and exclude other diagnoses. International guidelines have rightly placed great emphasis on the presence of typical cataplexy which, if present, in the context of EDS is sufficient for a positive diagnosis. Many authorities, however, would advocate obtaining objective evidence of sleepiness by undertaking a multiple sleep latency test (MSLT). Over four or five nap opportunities at two-hourly intervals, a narcoleptic should fall asleep, on average, within eight minutes or sooner and enter REM sleep within 15 minutes in at least two of the naps. These criteria have some validity although are very dependent on how the investigation is undertaken, its rigour and the precise protocol used. For example, monitoring of overnight sleep to ensure adequate sleep length before the MSLT is mandatory but often overlooked.
Table 3.1 A summary of questions that might help in diagnosing narcolepsy clinically.
| Probe for possible narcolepsy | Comments |
| Have you fallen asleep in particularly unusual situations? | Most narcoleptics will admit to unplanned naps in public, on buses for example. |
| Are you prone to losing objects around the house or performing inappropriate behaviours when ‘half asleep’? | Automatic behaviours during presumed ‘microsleeps’ are very common alongside frank sleep episodes |
| Do you find short naps restoring? | In contrast to many causes of severe EDS, narcoleptics often find a 20-minute nap restorative, allowing them a further period of useful wakefulness |
| Do you routinely dream in short daytime naps? | A positive answer implies that REM sleep is occurring soon after sleep onset, a very characteristic feature of narcolepsy |
| In general, are your dreams very vivid, bizarre or difficult to distinguish from reality? | Most narcoleptics report unusual or excessive dream activity with an unusually clear and persisting memory for vivid dreams or nightmares |
| Is your overnight sleep fragmented and of poor quality? | The majority of narcolepsy patients sleep very poorly overnight, either with spontaneous awakenings or intrusions of REM sleep phenomena and other parasomnias |
| Do you experience brief symptoms of weakness when emotional, particularly during laughter? | A very important question for exploring cataplexy which can be focal or subtle and confined to speech disturbance or head bobbing |
| Have you developed a craving for sweet foods in particular, perhaps overnight? | Increasingly, it is recognised that narcolepsy is associated with unusual eating habits or appetite control |
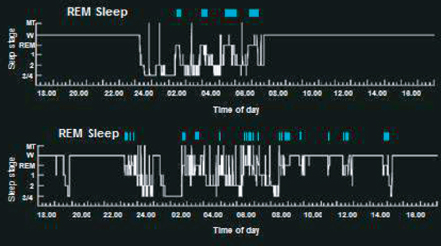
Overnight polysomnography in narcolepsy usually reveals poorly organised and fragmented sleep, often with an excess of movement, both in REM and non-REM sleep stages (Figure 3.2). An early onset of REM sleep within 20 minutes might also be seen. These changes are not specific, however, and may be influenced by concomitant medication.
Figure 3.2 24-hour hypnograms showing the distribution of wake and sleep across a full day and night for a control subject (top) and a narcoleptic (bottom). In the narcoleptic, there is a chaotic distribution of sleep across the night with frequent arousals. During the day there are several brief sleep episodes with REM sleep intrusions.