CHAPTER 7 EXECUTIVE FUNCTION AND ITS ASSESSMENT
EXECUTIVE FUNCTION
The dysexecutive syndrome has long been exemplified by the classic case of Phineas Gage, whose prefrontal damage from a railway construction accident in 1848 completely altered his personality and work performance.1 A more contemporary exemplar, with the advantage of modern neuroimaging and neuropsychological assessment, is that of E.V.R., reported by Eslinger and Damasio.2 E.V.R. was a successful young accountant who underwent surgical removal of a large orbitofrontal meningioma. His postoperative course illustrates the potentially far-reaching and devastating consequences of executive function impairment:
Characterization of Executive Function
Executive function can be understood as the skills that allow humans to solve problems; adapt effectively and flexibly to their environment; and plan, perform, and evaluate goal-directed intentions, such as making a timely financial investment. Correspondingly, executive dysfunction can lead to deficits in the generation and initiation of appropriate behavior, limitations in cognitive flexibility and reasoning skills, and impairments in social judgement.3–10 The breadth of coverage in these descriptions immediately signals the complexity of the processes involved and, not surprisingly, the difficulty that researchers have encountered in formulating adequate and comprehensive explanatory models of these behaviors.
Notwithstanding this challenge, executive function continues to be a focus of interest for both researchers and clinicians, because the concept provides a description of humans’ adaptability to their environment and assistance in developing expectations and predictions of relevance to (1) differential diagnosis in clinical evaluations (for example, in delineating the syndromes of the frontotemporal dementias; see Chapter 74); (2) anticipating dysfunctional behavior of patients in everyday settings11; and (3) estimating decision-making capacity in everyday roles (for example, capacity for handling financial responsibilities12). Understandably, assessment of executive function has become a core component of most neuropsychological assessments.13
Neuropsychological Models of Executive Function
Neuropsychological approaches to conceptualizing a model of executive function are varied. Banich4 provided a helpful roadmap to several of the approaches, including working memory, the supervisory attentional system, script knowledge, and goal-directed behavior. A brief description of two of the major theories follows.
Working Memory
Baddeley’s working memory model14 (Fig. 7-1) consists of multiple specialized and interlinked components of cognition that allow humans to (1) mentally represent their immediate environment, (2) retain information online (available in consciousness in an ongoing manner) to enable acquisition of new knowledge, and (3) formulate and act on current goals, through both an attentional control system—the central executive—and several specialized temporary storage systems, which are slave systems to the central executive, such as the articulatory loop and the visuospatial scratch pad.15 Working memory provides online cognition (manipulation of data in consciousness) that allows a reasoned response to complex tasks.
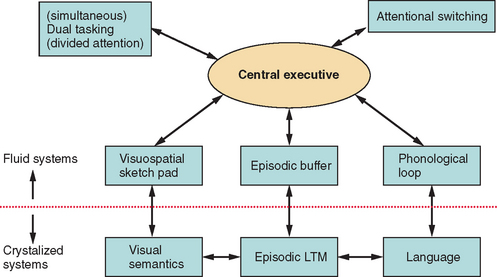
Research since the 1990s has consistently supported the proposition that the central executive can be fractionated, or, as Baddeley persuasively commented, skills can be governed by an “executive committee” rather than a “homunculus.”16 There have been various attempts at defining the breadth and nature of executive functions.16–18 However, most taxonomies include focusing attention and inhibiting distraction, coordinating and dividing attention, switching attention, planning, and activating and generating representations drawn from long-term memory via an episodic buffer. Impairments in working memory can result in many of the core features of executive dysfunction, such as inability to maintain task focus as a result of susceptibility to distraction, or inability to perform two or more tasks simultaneously (multitasking). (An example of such multitasking would be simultaneously monitoring young children playing in a swimming pool and cooking a meal, while speaking on a mobile phone.)
Working memory, therefore, can provide a comprehensive account of many features of executive dysfunction. Furthermore, the executive aspects of working memory have been closely associated with the prefrontal regions, especially the dorsolateral prefrontal cortex.19
Supervisory Attentional System
Within this model, the emphasis is on the role of attentional control (executive function) in everyday actions. Shallice20,21 provided a two-layer model of an attention system that influences behavior: contention scheduling (automatic processing) and the supervisory attentional system (controlled processing). Contention scheduling allows fast automatic execution of well-learned action sequences. This may be sufficient for many everyday tasks, but it is also prone to error as it operates under minimal conscious supervision. For example, making a cup of coffee can become relatively automatic, but sometimes when a person is tired or distracted, he or she may unintentionally pour milk into the coffee pot instead of into the cup. In contrast, the supervisory attentional system is activated when conscious effort is required: for example, in situations of novelty or crisis or when new skills are learned. An impaired supervisory attentional system and an unmonitored contention scheduling system can account for many of the qualitative features of executive dysfunction, such as perseveration (failing to cease an ongoing behavior when it is no longer appropriate).
Contention scheduling and the supervisory attentional system have been proposed to be operated by distinct neural substrates. Specifically, the supervisory attentional system is associated with the prefrontal cortex.22 Initially, the supervisory attentional system was conceptualized as a unitary construct, but more recently, Stuss and Alexander argued for a multicomponent supervisory attentional system within which specific processes interlink with specific neural substrates of the frontal cortical-subcortical neural network.10 Furthermore, Stuss and Alexander cautioned against a simple conceptualization of supervisory attentional control. They emphasized that there are many types and levels of attentional control of behavior (e.g., Fig. 7-2) and that the concept of a simple frontal/posterior dissociation related to control/automatic processes would not adequately capture the complexity of linkage of the system to particular neural substrates. They thereby concurred with other authorities that executive function fractionates into various subordinate roles important for goal-directed behavior.
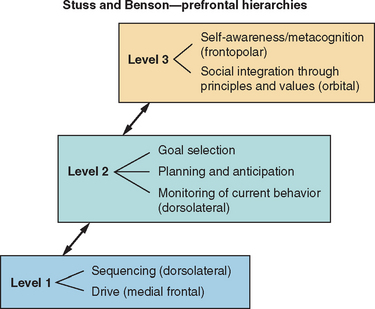
Figure 7-2 Diagrammatic representation of model of executive function.
(From: Stuss DT, Alexander MP, Benson DF. Frontal Lobe Functions. In Trimble MR, Cummings JL, eds: Contemporary Behavioral Neurology. Boston: Butterworth Heinemann, 1996, pp 169-187.)
Although varied, existing theories of executive function are not necessarily mutually exclusive. Within most models, there is recognition of a multicomponent executive function system subserving multiple roles. Furthermore, although executive function disorders are more commonly observed with frontal system dysfunction, most researchers argue that it would be overly simplistic to reduce executive function to a concept of frontal lobe disorder; instead, executive skills undoubtedly rely on networks of interactive systems.10
Neuroanatomical Substrates of Executive Functioning
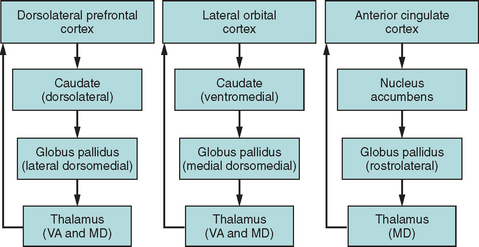
Functional imaging studies have confirmed that complex behaviors such as executive functions are subserved by networks of interconnected brain regions rather than by discrete cortical areas (Fig. 7-3), and a series of parallel frontal-subcortical circuits that link specific regions of the frontal cortex to the striatum, globus pallidus, and thalamus have been described.23,24 Miller and Cummings provided an extensive model of five defined frontal-subcortical circuits,25 of which the dorsolateral prefrontal, orbital frontal, and anterior cingulate circuits are purported to subserve cognitive and behavioral aspects of executive function.26 A corollary of this network structure is that interruption of such circuits outside the frontal cortex leads to many of the classic features of “frontal” dysfunction. For example, infarcts in the caudate head may disturb planning and sequencing, with disinhibition or apathy, depending on which part of the caudate—and therefore which circuit—is disrupted (e.g., see Mendez et al27). Progressive supranuclear palsy is another example of a disorder whose pathological effect is subcortical rather than on the prefrontal cortex and yet that is characterized by a prominent dysexecutive syndrome on the basis of disruption of these circuits.28
Orbitofrontal Circuit
The orbitofrontal circuit is important for inhibition, and changes in this control mechanism can, in a variety of ways, affect the behavioral response to environmental and social demands.24,26 Affected patients have been described as acting impulsively, exhibiting emotional and socially inappropriate behavior, and being liable to increased distractibility.29 In severe instances, dysfunction can result in the phenomenon of utilization behavior, in which patients become devastatingly stimulus-bound to environmental cues.30 The orbitofrontal network serves as a braking mechanism to stop automatic responding and allows for a flexible approach to environmental manipulation.
Anterior Cingulate Circuit
The anterior cingulate circuit is medial in location and has been implicated in resistance to interference (including cognitive inhibition of automatic responses) and in response initiation.31 Cummings24 described the characteristic syndrome as that of apathy, the most extreme form being of akinetic mutism: a profound indifference to the environment in which patients lack any internally generated activity or behavior (see Chapter 9).
Dorsolateral Prefrontal Circuit
Impairment of the dorsolateral prefrontal circuit is argued to contribute to many of the observed cognitive features of executive dysfunction that affect cognitive flexibility or attentional switching and the formulation of novel ideas and responses. Deficits include impairments in self-generated behavioral (motor or cognitive) planning, maintenance of cognitive set and set switching,9 and manipulation of working memory information online.32 Patients with dorsolateral lesions are frequently described as displaying impaired mental flexibility and poor reasoning.
Information Flow to the Frontal Cortex
A complementary view of executive functioning and the prefrontal cortex is that the dorsolateral prefrontal cortex sits at the apex of information flow from the external milieu (the subject’s interaction with the external environment), after that information has been processed through unimodal and then multimodal association cortices, and is able to modulate and select responses to this information. The orbitofrontal and mesial prefrontal cortices, in contrast, receive information on the subject’s internal milieu, including needs and drives, and modulate and select responses to these stimuli.33,34
Therefore, although there is continuing debate on a comprehensive taxonomy of executive processes, most researchers agree that executive function is a fractionated functional system that relies on differentiated underlying neural regions and pathways.
FORMAL ASSESSMENT OF EXECUTIVE FUNCTION
Common Problems Affecting Executive Function Tests
Most clinicians are familiar with the frustrating situation in which patients with executive dysfunction have a significant discrepancy between the reasonably average results of formal testing procedures and major difficulties in real-life behavior.6 Sometimes this may relate to the following aspects of the testing process.
Repeated Testing Can Lead to Marked Practice Effects
All executive function tests suffer from practice effects. Although parallel test versions may be available to obviate direct learning effects of the test material (for example, alternate letters in verbal fluency), procedural learning (implicit learning that can improve performance simply by performance of a task more than once) is common in executive function tests. This may reflect the fact that the tasks are designed to be novel and cognitively engaging and the fact that the participant will actively attempt to rehearse strategies to make the task easier. With repeated exposure, a previously novel task therefore becomes automatic.35 This represents a major difficulty in longitudinal studies.
Testing in the Office Is Not the Same as Real-Life Situations
In formal testing procedures, most typically conducted within a quiet office environment, distractions are minimized, and tasks are often carefully structured to increase the reliability of the test. However, these artificial constraints may substitute for the patient’s defective executive system.36 Furthermore, test procedures can be relatively brief episodes, so that persistent and sustained attention to a task is rarely assessed thoroughly, and demand for multitasking is low.6,13,37 Unfortunately, these constraints of office testing can prevent the demonstration of the essential features of executive dysfunction. To improve the ecological validity of the assessment, formalized versions of real-world activities in which patients are assessed in naturalistic settings (e.g., Shallice and Burgess’s shopping center task9) have been devised; although these approaches have yielded highly informative results for guiding rehabilitation,38 they are generally impractical for a busy hospital-based assessment clinic.
Assessment of the Affective, Social, and Judgmental Changes of Executive Dysfunction Are Not Well Covered by Existing Tests
Alterations in emotional and social behavior are important components of the executive syndrome, to the extent that Stuss and Alexander argued that social behavioral changes represent the most disabling aspect of the disorder.10 Performance on many tests can be undermined by apathy, disinhibition, or other features of lack of emotional control. However, formalized approaches to the documentation of these key characteristics are limited, although research measures of social cognition, such as the faux pas test,39 or of judgment, such as the gambling game,40 show promise.
Level of Premorbid Ability Is Important when Executive Function Is Assessed
It is important to evaluate executive function within the context of the estimated overall premorbid ability of the individual; that is, a below-average score on a test of executive function may be significant if the patient was of above-average premorbid ability, but it would be less suspect if previous general ability was estimated to lie in the below-average range. Furthermore, researchers41,42 have noted that tests of executive function are frequently correlated with general cognitive ability in healthy populations, and this should be considered when individual performances in tests of executive skills are evaluated.
Standard Neuropsychological Tests Commonly Used in Assessing Executive Function
Test Batteries or Individual Tests for Executive Function?
There are now several test batteries of executive function, including the Behavioural Assessment of the Dysexecutive Syndrome (BADS),43 the Behavioral Dyscontrol Scale,44 and the Delis-Kaplan Executive Function Scale (D-KEFS).45 The D-KEFS is especially useful because of its reasonably large normative sample and the provision of multiple standardized tests in which the same outcome scale is used for comparison purposes. These batteries should be considered for use, because they allow comprehensive assessment of executive function; however, in many clinical examinations, time is limited and administration of a full test battery cannot be easily accommodated. Consequently, the neuropsychologist is faced with the decision of individual test selection.
Consideration of the cognitive and neural models of executive function, and of reports of the patient’s particular difficulties, is essential to guide the examiner in determining which aspects of the fractionated roles of executive function are critical in the assessment. The following sections summarize some of the neuropsychological tests commonly used to assess executive function. The listing is by no means exhaustive, and for more information on these and other related tests, the reader is referred to Lezak and colleagues (2004). The listing of the tests within separate domains of executive function is also debatable16,17 and is provided simply as a guide to the reader. As stated earlier, neuropsychological tests of executive function tend to be multifactorial, which precludes a simple description of the underlying properties of the tests.
Focusing Attention and Inhibiting Distraction
An important feature of executive function is the ability to maintain attention on task and to resist interference from distracting events or thoughts. The Stroop Test46–49 provides a classic paradigm for assessing capacity to resist interference from an automatic process (in this instance, reading words: the names of colors) on a more effortful process (identifying the colors of the ink in which the words are printed). There are multiple versions of this test (including the Color-Word interference subtest from the D-KEFS), but in the basic task, participants are timed in (1) reading aloud words that are the names of colors; (2) naming ink patches of color; and (3) naming the color of the ink in which incongruent-color words are printed: for example, stating “blue” when the word “red” is printed in blue letters.46 The increased time taken to complete this final interference trial provides an index of the capacities to focus attention on the appropriate stimulus and to inhibit distraction from the more automatic response of reading the color word (cognitive inhibition). Excessive slowing or an increase in errors on the interference trial provides indication of diminished ability to inhibit inappropriate responses (Fig. 7-4). The test is relatively quick to administer (most versions take approximately 8 minutes), and scoring is by time or error on each trial. A substantial amount of cognitive neuropsychological research50 and a number of neuroimaging studies have confirmed the role of executive function and of the prefrontal regions of the brain—specifically, the anterior cingulate/mesiofrontal circuit—in task performance.51,52
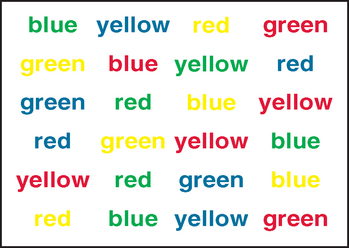
Figure 7-4 Interference trial of the Stroop test (Victoria version).
(From Spreen O, Strauss E: A Compendium of Neuropsychological Tests: Administration, Norms and Commentary, 2nd ed. New York: Oxford University Press, 1998.)
Satisfactory test-retest reliability has been reported for different test versions;6,53 for example, Houx and associates reported high test-retest reliability (r = .80) within a multicenter study of 5804 older adults.35 However, practice effects, as observed in most executive measures, are apparent. Houx and associates reported that speed of performance on the interference trial improved by approximately 5 seconds between baseline and reassessment 2 weeks later, and they argued that procedural learning in the Stroop test has to be taken into account when the course of executive function in patients is monitored over time. Impaired visual acuity or severe color blindness precludes use of the test, but it has been found to be sensitive to executive dysfunction in a range of clinical populations, including patients with traumatic brain injury54 and mildly and moderately demented patients.55 In both of these populations and in patients with Huntington’s disease,56 however, increasing severity of disorder results in increased generalized slowing of response, so that the specific Stroop effect diminishes.55,57 More recent versions of the test have increased its complexity by adding an additional switching trial to the basic color naming, word reading, and color-word interference trials.54,58,45,54 In the switching trial, participants are required to name the color of the ink as per the traditional color-word interference trial but to switch to reading the color word of any items enclosed by a rectangle, randomly positioned throughout the trial. This addition provides increased sensitivity for the identification of mild impairment in executive function.
Set-Shifting and Cognitive Flexibility
The ability to shift attention readily between different cognitive tasks (cognitive flexibility) is an important feature of adaptive behavior.16,58 One of the most popular tests of set-shifting is the Trail Making Test (TMT)59,60 which consists of two parts: the Trail Making Test Part A (TMT-A) and the Trail Making Test Part B (TMT-B). The TMT-A is a timed trial that requires participants to draw lines to interconnect 25 consecutively numbered circles. The TMT-B is also timed and requires participants to interconnect consecutive numbers and letters, alternating between the two sequences (i.e., 1-A-2-B-3-C-4-D …. L-13). Scoring is based on time to complete each trial (errors being reflected in the time score) and derived scores of (1) the difference in time to complete the two sections (TMT-B score minus TMT-A score) and (2) the ratio of TMT-B score to TMT-A score. The derived scores provide the advantage of removing the individual variance in speed of response before set-shifting capacity is calculated. These derived scores, as well as time taken to complete TMT-B, have frequently been used as indices of cognitive flexibility or set-shifting.61–66 The derived scores have been shown in some reports of TMT performance to provide better correlations with other measures of cognitive flexibility,61 and neuroimaging research has provided support for the critical role of the dorsolateral and medial frontal cortices in the regulation of cognitive flexibility and set-shifting, as required in the TMT.67
The TMT is quick to administer (approximately 4 to 6 minutes), but additional difficulties in visual scanning and motor control can compromise performance. To address this, the TMT subtest in the D-KEFS includes three extra conditions that allow the contributions of visual sequencing and motor speed to be evaluated more thoroughly.45 Because the TMT is predicated on familiarity with the English alphabet, the Color Trails Test68 was developed to provide a nonalphabetical parallel form for use in cross-cultural studies or clinical settings, although only limited normative data are available.69,70
Satisfactory test-retest reliability is reported for the TMT, with many reported coefficients higher than .80 and all exceeding .60.6,53 However, practice effects are again noticeable, especially on the TMT-A, and need to be considered when performance over time is evaluated. A large normative study of 911 participants aged 18 to 89 years has provided useful information on the TMT-A and TMT-B and on the effects of age and education on test performance,71 and this can be supplemented by normative information on the derived scores from a smaller study.72
The TMT has been demonstrated to be sensitive to cognitive impairment in a range of clinical conditions, including Parkinson’s disease,73,74 Alzheimer’s disease,75,76 and other dementias.77–81
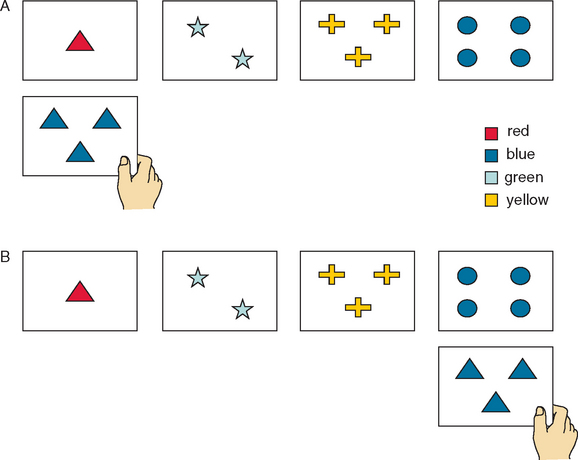
The WCST82,83 is the most extensively characterized test of executive function. Although multifactorial, it is frequently described as a task of attentional set-shifting.17,84 The test requires the client to sort a set of cards on the basis of several different characteristics: color, form, and number. Clients are not given instructions on how to sort the cards but must infer the correct method of sorting from the examiner’s mention of “Correct” or “Incorrect” in response to their previous sorting attempts (Fig. 7-5). After a series of consecutive successful sorts, the sorting principle changes without notice, and the participant must both discern that the rule has changed and discover the new criterion for sorting. Scoring includes the number of correct categories achieved and the number of perseverative errors (an error of sorting within a category that was formerly correct but is no longer appropriate: that is, a failure in ability to switch response according to task demands).
< div class='tao-gold-member'>





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


