Chapter 168 Explant Analysis of Wear, Degradation, and Fatigue in Motion Preserving Spinal Implants
Because of their rarity, certain failure modes may escape detection in a clinical trial. For this reason, the U.S. Food and Drug Administration (FDA) is keenly interested in the detailed analysis of explanted implants, as evidenced by the inquiry and recommendations of three FDA panels for cervical and lumbar artificial discs from 2004 to 2007. In the 2007 FDA panel meeting for the Bryan cervical disc (Medtronic, Memphis, TN), one of the conditions for approval was that the manufacturer conduct a 10-year postmarket retrieval analysis of the device (www.fda.gov/cdrh/meetings/071707-summary.html). Retrieval analysis is considered an absolutely essential companion activity not only for prospective, randomized clinical trials but also for the postmarket surveillance of new spinal implant designs.
Retrieval analysis has strong regulatory and societal implications and is performed by clinicians, engineers, and biologists. There are great advantages from their collaboration as a team, which allows for the relevant patient-related, surgeon-related, and implant-related factors to be considered in as broad a context as possible. When properly performed by experienced investigators, retrieval analysis can provide a definitive source of information on implant-related and biomaterial-related failure modes, biocompatibility, and their impact on the overall longevity of the surgical procedure. When compared with the findings of experimental or numerical studies, the results of retrieval analysis can help validate preclinical testing and computer-based methods that are essential when evaluating new designs. Taken one step further, when the aggregate results of retrieval analysis are integrated into the implant design process, the technique can provide feedback or motivation for adjusting implant designs or finding alternative biomaterials. As explained in a consensus statement from the National Institutes of Health,1 “Technology progresses by facing its failures and learning from its successes. The goal of device research and development is to improve patient care through improvement of implants. A fundamental objective is to understand successful implants and assess failures through retrieval analysis.”
There is also strong educational and ethical motivation for participating in retrieval analysis. When involving researchers, engineers, and clinicians in the early stages of their careers, retrieval analysis has a major educational component. Clinicians who are actively implanting motion preserving devices have an ethical responsibility to contribute to retrieval analysis to provide their patients with the best care possible. The removal of an implant, especially a lumbar artificial disc, exposes the patient to increased risk of serious, potentially life-threatening complications. The clinician has a responsibility to ensure that implanted and explanted devices and tissues are properly analyzed and the results disseminated to stakeholders. There are many scientific, educational, and ethical reasons why the research community, implant designers, and surgeons are motivated to participate in retrieval analyses. These reasons have been touched on in previous review articles and book chapters.2 It is a testament to the varied and compelling motivations for retrieval analysis that it continues to play an important role in the evolution of implant technology.
Practical Aspects of Retrieval Analysis
Retrieval Program
A retrieval program may be organized as the collection and analysis of implants from a single institution or from a multi-institutional study or independently as a more generalized retrieval repository. When a retrieval program is established as part of a clinical study, institutional review board approval or the equivalent should be obtained, which may require the informed consent of each patient to participate. A clinical study–type design is preferred when detailed clinical information, including protected health information, is being collected and analyzed as part of the study. Details on the design and establishment of a retrieval or repository program have been outlined previously.3
To ensure adequate receipt and processing of the retrieved implants, standard precautions should be used when handling the explanted components until they have completed a cleaning protocol. These precautions may include keeping the implant components in appropriate chemicals to preserve adhering tissue (e.g., formalin), provided that the preservative does not degrade the component itself. At our center, implants fabricated from titanium alloy, cobalt chromium (CoCr) alloy, and polyethylene are ultrasonically cleaned in soap and deionized water, rinsed, and sterilized using a 10% bleach solution. We omit the bleach solution for cleaning stainless steel implants because there is the potential for corrosion. Likewise, a mild cleanser is used for implant components composed of polymers that may be vulnerable to chemical changes from a bleach solution. Additional guidance for handling of retrieved implants and tissues may be found in American Society for Testing and Materials (ASTM) Standard F561.4
The analysis of retrieved implants and tissues may involve a broad range of test methods, which are comprehensively described in ASTM Standard F561.4 This manual provides guidance for analysis of all implant components, including metallic, polymeric, and ceramic materials. Although a detailed summary of this standard is beyond the scope of this chapter, we highlight in subsequent sections specific test methods that have been particularly helpful in the characterization of retrieved metal-on-polyethylene and metal-on-metal disc replacements.
Wear and Damage Assessment
Because wear and damage of retrieved TDRs can occur at length scales that are invisible to the naked eye, microscopy may be necessary to identify damage modes. An optical stereomicroscope, with 10× to 40× magnification, is typically sufficient to identify worn regions of retrieved implants, but frequently it is helpful to analyze the wear surfaces using scanning electron microscopy (SEM), achieving magnifications of 5000× or greater. In addition to optical and SEM, micro-CT and white light interferometry (WLIR) are two methods that have proven particularly useful in our previous analyses of wear in retrieved TDR and dynamic stabilization components.3,5–7 These novel wear assessment methods are highlighted in this section.
Micro-CT Analysis
We have used a micro-CT to detect nondestructively surface and internal voids and cracks within retrieved polyethylene TDR components5 and polyurethane motion preserving spinal implants.7 Depending on their thickness, CoCr alloy components produce substantial artifacts on micro-CT. Consequently, we have found it helpful to remove the wire marker before micro-CT analysis of rim wear in the Charité design. The removal of the wire marker for other analyses may be unnecessary because the artifact does not extend into the central core of the implant. For polymer components that do not incorporate wire markers (e.g., ProDisc [Synthes, Paoli, PA] or Dynesys [Zimmer Spine, Minneapolis, MN]), micro-CT artifacts are not an issue.
At the authors’ institution, polymer components of motion preserving spinal implants are scanned at 18 μm voxel resolution using a commercial micro-CT scanner (μCT80, Scanco Medical, Bassersdorf, Switzerland).5 The three-dimensional reconstructions of the component and two-dimensional sections taken through the component are evaluated for the presence of surface, through-thickness, and internal voids or cracks. Previously, we have observed the trajectory of cracks in polymer components of motion preserving spinal implants, including Dynesys.7 Using optical microscopy, we have also characterized permanent deformation and wear patterns of polymer components from motion preserving spinal devices. Using these methods, we have been able to distinguish these forms of surface and subsurface damage from iatrogenic damage that occurs during implant removal.
Because of attenuation artifacts encountered with metallic components, micro-CT is useful only for polymeric components from TDRs. To measure the macroscopic surface geometry of metallic components, tools employed by the research community include coordinate measurement machines, laser profilometers, and optical profilometers. To measure microscopic changes in the implant surface, WLIR may be used. As discussed next, interferometry is applicable to both metallic and polymeric components of disc replacements.
White Light Interferometry
We use WLIR to characterize the microscopic surface morphology of retrieved disc arthroplasty components. WLIR is capable of detecting surface height changes that are on the nanometer length scale by measuring the interference of white light reflected off the component within a specified field of view compared with the light from a reference beam. We have successfully analyzed the wear surfaces of polyethylene and CoCr alloy TDRs at our institution using a NewView 5000 equipped with advanced texture analysis software (Zygo, Middlefield, CT).6 We sample 5 to 10 square regions (typically 0.54 × 0.72 mm) of a component to obtain representative surface topography of the retrieved implant in both worn and unworn locations.
Figures 168-1A and B illustrate the surface topography obtained from unworn and worn surface regions of a retrieved polyethylene disc replacement component that was implanted for 12.7 years. The unworn polyethylene surface is dominated by machining marks that are on the order of several microns in amplitude (see Fig. 168-1A). Initially, microscopic evidence of adhesive and abrasive wear is detected by the erosion and removal of machining marks, along with the presence of fine scratches (see Fig. 168-1B).
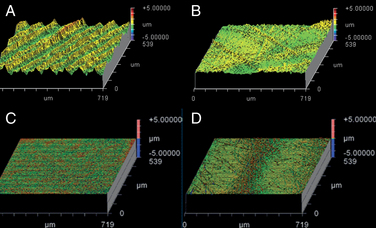
The surface topography of a retrieved CoCr alloy disc replacement is shown in Figures 168-1C and D. The unworn CoCr surface is usually relatively flat and featureless, aside from microscopic scratches generated during the final polishing stage of the manufacturing process (see Fig. 168-1C). In a region of wear, the CoCr surface has evidence of localized, microscopic scratches with a characteristic length scale that is larger than the residual features from polishing (Fig. 168-1D).
As shown in Figure 168-1, surface characterization using WLIR provides useful information about the wear mechanisms in TDRs. In addition, by quantitatively analyzing the surface data, the roughness and waviness can be quantified and compared with as-manufactured components, providing insight into the magnitude of surface changes or wear that occur in vivo.8–10 Ultimately, quantitative measurements of implant surfaces are used to validate in vitro and computational models that seek to simulate in vivo wear processes.
Wear and Damage Mechanisms
As discussed in the previous section, metal and polymeric components from retrieved motion preserving spinal devices should be evaluated macroscopically and microscopically for the presence of damage modes typically observed in large joint arthroplasty components (e.g., burnishing, abrasion, scratching, pitting, plastic deformation, fracture, fatigue damage, and embedded debris). A detailed description of wear and wear mechanisms is beyond the scope of this chapter and can be found in books dedicated to this subject.11 A generic guide for the analysis of retrieved components is summarized in the Appendices for ASTM Standard F561.4 This section provides a concise summary of the most relevant wear and fatigue damage modes that may be encountered when inspecting retrieved motion preserving spinal implant components.
Abrasion and Scratching
Abrasive wear is evidenced by scratching and is common to both metallic and polymeric components for TDR. Abrasion may be apparent macroscopically by the naked eye, or it may be apparent only when viewed using microscopy. Abrasive wear occurs when microscopic surface irregularities (also referred to as “asperities”) in one implant scratch the surface of the opposing counterface. In the case of metal-on-polyethylene, the asperities on the metallic implant produce scratches in the softer polymeric implant. In the case of CoCr alloy metal-on-metal implants, abrasive wear is produced by locally stiffer asperities, such as carbides, plowing through the relatively softer cobalt alloy matrix. Abrasive wear can also occur when softer polymeric components of the implant contact surrounding bony structures (Fig. 168-2).
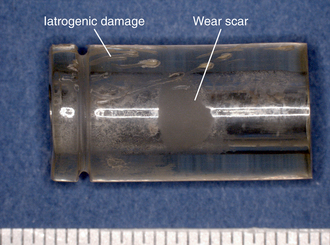
FIGURE 168-2 Abrasive wear observed on polymeric components from retrieved Dynesys systems, implanted 1.1 years.
During retrieval analysis, the pattern of scratches on an implant, whether macroscopic or microscopic, provides clues to the kinematics (motion) of the surfaces while they were contact in vivo. The microscopic multidirectional scratches and crisscrossing wear paths at the dome of a retrieved polyethylene TDR (Fig. 168-3) are consistent with the type of microscopic abrasive wear mechanisms previously observed in retrieved hip replacement components.12,13 By matching comparable regions of damage on two opposing bearing surfaces, it is further possible to infer the orientation of the components while they were in contact.

Burnishing
Typically encountered with polyethylene disc components, burnishing gives the polymer surface a polished, glossy appearance (Fig. 168-4). At a microscopic length scale, burnishing is associated with an adhesive wear mechanism, whereby the polyethylene surface wear occurs by adhesion to the metallic counterface. Magnified images of a burnished wear zone from a retrieved TDR are shown in Figure 168-4 and as noted also show evidence of scratching, which denotes the presence of abrasion. For this reason, the dominant wear mechanism in metal-on-polyethylene articulations is considered to be a combination of adhesion and abrasion, as seen in total joint replacements.12,13
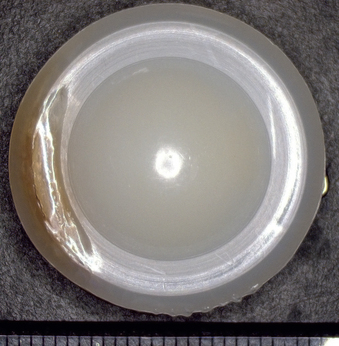
FIGURE 168-4 Burnishing observed on the dome of the polyethylene component of a retrieved total disc replacement.
Surface Deformation
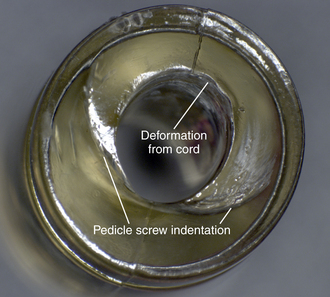
In motion preserving spinal devices, macroscopic surface deformation has been observed in components that undergo compression in vivo. Polycarbonate urethane (PCU) spacers used in the Dynesys system undergo deformation owing to cold flow of the material, the compressive load applied during the surgery, and subsequent loading in vivo, which results in permanent bending of the implant and indentations from the supporting polyaxial screws (Fig. 168-5). Additional deformation of soft polymer components may occur from interaction with other components from the implant, for example, the cord component that passes through the center of the polyurethane spacer in the Dynesys system (see Fig. 168-5).
Fatigue Wear and Fracture
Fatigue wear and fracture, especially of the rim, are a concern with polyethylene TDRs. David et al.14 reported a case in which the entire rim of a disc replacement fractured from the central body of the core after 9.5 years in vivo. This case of rim failure was attributed to severe oxidation degradation after gamma sterilization in air.
The severity and clinical manifestation of fatigue-related rim damage in the Charité design varies widely, ranging from full-thickness transverse rim fracture (Fig. 168-6) to more benign radial crack formation (Fig. 168-7). In our retrieval studies of the Charité, radial cracks have been observed in 27 of 53 implants examined so far.15 Similarly, transverse cracks have been observed in 17 of 53 retrieved implants.15 In most cases, fatigue fracture is related to impingement by the metallic end plates. Fractures have also been observed in polymer components of dorsal devices such as the Dynesys (Fig. 168-8).
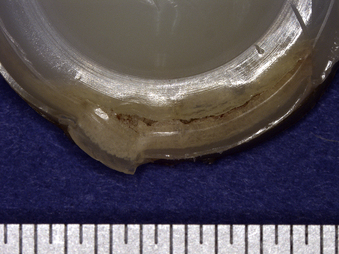
FIGURE 168-6 Fatigue-related rim fracture observed in a retrieved Charité implant that was implanted for 9.2 years.
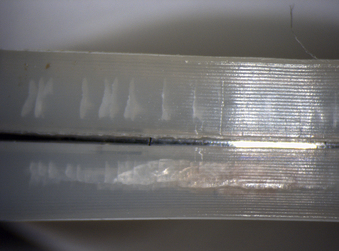
FIGURE 168-7 Fatigue-related radial rim cracking observed in a retrieved Charité prosthesis that was implanted for 3.1 years.
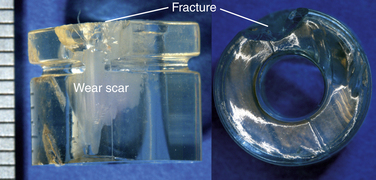
FIGURE 168-8 Optical microscopy of a fatigue-fractured spacer from a retrieved Dynesys system that was implanted for 1.1 years.
Related posts:
 Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


