Chapter 1 Extradural Benign Tumors
VERTEBRAL HEMANGIOMA
EPIDEMIOLOGY
• Hemangiomas are benign, slow-growing skeletal and soft tissue tumors that commonly involve the bony spine.
• The actual incidence of hemangiomas is uncertain as they are often discovered only incidentally in asymptomatic individuals. They account for approximately 2–3% of all spinal tumors and occur with an estimated incidence of 10–12% in the population as based on large autopsy series and review of plain spine radiographs.1
• These lesions are usually asymptomatic and often present as incidental findings on plain radiographs and on magnetic resonance (MR) images.
DISTRIBUTION
• Vertebral hemangiomas are extremely vascular bone tumors. They commonly occur as incidental findings within the vertebral body.2
• Vertebral hemangiomas are the most common benign spinal neoplasms. The peak incidence is in the fourth to sixth decades, with a tendency to increase in size with age.3,4
• Asymptomatic hemangiomas occur equally in men and women, but there is a female predominance with symptomatic lesions. Symptomatic hemangiomas (about 1% of all hemangiomas) are usually observed during adult age and tend to occur in the thoracic region.5
• Pregnancy may exacerbate vertebral hemangiomas.2,3 Vertebral hemangiomas are solitary in 66% and multiple in 34% of cases.4
• These tumors have a predilection for the thoracic spine (60%) compared with the lumbar spine (29%), cervical spine (6%), and sacrum (5%).4 Concomitant posterior element involvement can be seen in 10–15% of cases.
HISTOLOGY
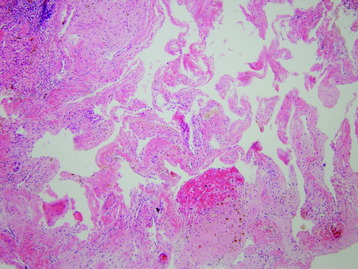
• Hemangiomas are composed of a collection of irregular vascular spaces lined by bland endothelial cells (Fig. 1-1).
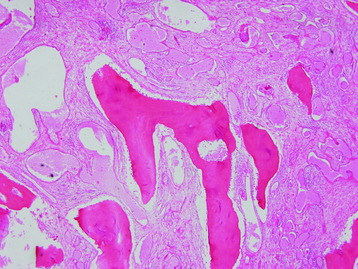
• They are slow-growing hamartomatous proliferations of vasogenic and endothelial tissue in the bone and can be of capillary or cavernous type; the latter is a more common type (Fig. 1-2).6
• Vertebral hemangiomas vary predominantly from fatty lesions to those composed largely of vascular stroma with little or no fat tissue.3
RADIOLOGY
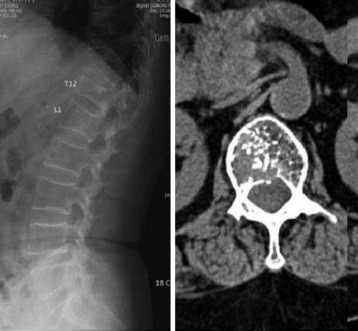
• On plain films, the thickened vertical trabeculae of hemangiomas cause parallel linear densities described as having “jail bar” or “corduroy” appearance, or may show lytic foci with honeycomb trabeculations.3 The classic “honeycombing” or vertically oriented vertebral lucencies separated by thickened trabecular bone are indicative of a vertebral hemangioma (Fig. 1-3).
• On axial computed tomography (CT), these thickened trabeculae give a typical spotted or “polka dot” appearance to the vertebral body (Fig. 1-4).

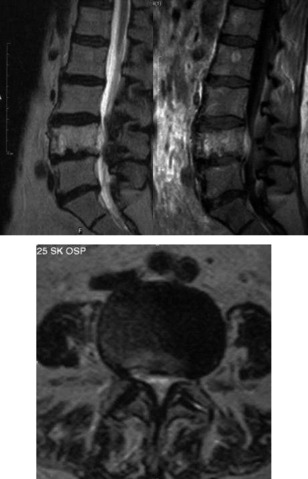
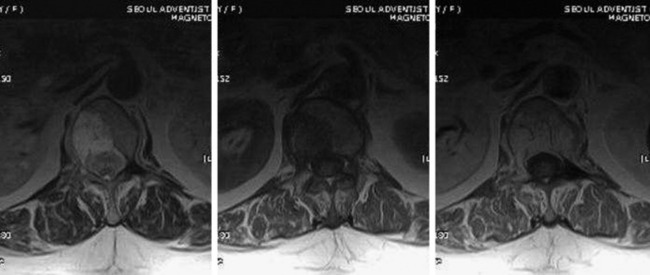
MR is extremely sensitive in detecting spinal hemangiomas. On both T1- and T2-weighted images, these lesions tend to have increased signal intensity, reflecting the adipose tissue rather than the hemorrhagic component. The hyperintense stroma surrounds foci of very low signal intensity, which represent the thickened vertical trabeculae (Fig. 1-5).3 In cases of hemangiomas that are rich in vascular element, the signal change is high on T2-weighted images (T2WI), low on T1-weighted images (T1WI), and shows homogenous enhancement with contrast (Figs. 1-6 and 1-7).

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


