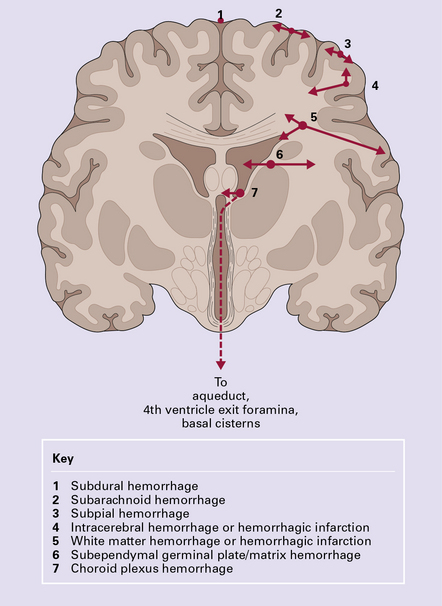
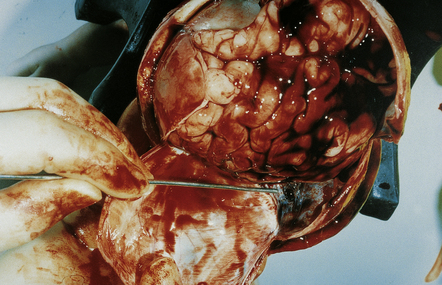
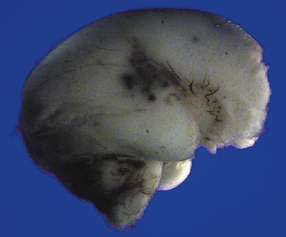
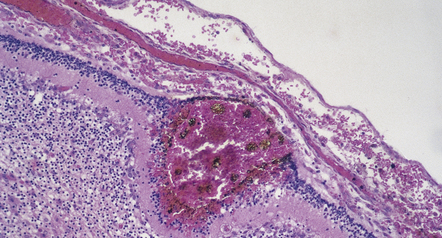
2 Possible pathophysiologic schema Principal factors involved in the production of lesions: Present knowledge of embryology and developmental physiology allows a tentative chronology to be assigned to individual lesions (Fig. 2.1) although this remains relatively imprecise and extreme caution is needed in the forensic arena. Although some pathologic changes closely parallel those found in older individuals, others such as intraventricular hemorrhage, white matter necrosis, and marbling are unique to the perinatal period. 2.1 A timetable for hypoxic–ischemic lesions in early life. MACROSCOPIC AND MICROSCOPIC APPEARANCES Much of the cerebral mantle is replaced by a thin translucent membrane. The hemispheres are cystic, and lack surface convolutions (Fig. 2.2). Inferior aspects of the temporal, occipital, and frontal lobes are usually spared, but sometimes only the hippocampi remain. The deep gray nuclei may be rotated outwards and the thalami are atrophied. The membranous cerebral mantle comprises an outer connective tissue layer and an inner irregular glial layer which also contains mineralized neurons, debris, and hemosiderin-laden macrophages. The ependyma is usually absent. At the interface with surviving cerebral tissue, the inner glial layer runs into the molecular layer, covering it for a short distance, while adjacent cortex is usually disorganized, often with a pattern of polymicrogyria (Fig. 2.3). This histologic appearance clearly distinguishes hydranencephaly from the macroscopically similar bubble brain in Fowler syndrome (see Fig. 7.2). 2.2 Hydranencephaly in a twin of 22 weeks’ gestation whose co-twin died at 17 weeks. MACROSCOPIC AND MICROSCOPIC APPEARANCES A porus is a smooth-walled defect in the cerebral mantle, usually surrounded by an abnormal gyral pattern. It varies in depth from a slight indentation or fissure to a full-thickness breach of the hemispheric wall connecting subarachnoid space with ventricle. Pori tend to be bilateral, approximately symmetric, and situated over the Sylvian fissures or central sulci. Unilateral defects may be parasagittal, orbital, or occipital, and associated with abnormal convolutions, especially polymicrogyria, which are symmetrically placed in the contralateral hemisphere. Gyri surrounding the defect form irregular or radiating patterns (Fig. 2.4). The cortex around the porus is broken into islands or folded into polymicrogyria, which extends down into the cleft to meet the ventricular wall. The latter is denuded of ependyma, but covered by glial tissue, which extends a short way over the adjacent gray matter (Fig. 2.5). Subependymal nodular heterotopia (Fig. 2.6d) and partial or complete absence of the septum pellucidum are other features. 2.4 Porencephaly. 2.5 Porencephaly. 2.6 Schizencephaly. Extensive bilateral porencephalic clefts (Fig. 2.6) are sometimes termed schizencephaly, especially in the radiologic literature, although the term schizencephaly refers back to an outmoded concept of circumscribed growth failure of the cerebral wall. The narrowness of the cleft with either closed or open lips was thought to differentiate malformed from acquired lesions, but clinical, morphologic, and experimental evidence favors a destructive origin for most lesions. There is also recent evidence for familial occurrence of schizencephaly in brothers with defects in the homeobox gene EMX2. In contrast to the smooth-walled defects of hypoxic–ischemic lesions of early gestation, third trimester insults produce many cysts throughout large areas of cerebral white matter and deeper cortical layers (Figs 2.7, 2.8). Occasional cases are unilateral and circumscribed (Fig. 2.9), but most are extensive and bilateral. Bilateral multicystic encephalopathy is often associated with cystic necrosis in the basal ganglia and brain stem tegmentum (Fig. 2.10). 2.7 Multicystic encephalopathy in a smaller first twin at 36 weeks’ gestation. 2.8 Multicystic encephalopathy. 2.9 Unilateral circumscribed form of multicystic encephalopathy. A meshwork of thin gliovascular septa form numerous cysts containing lipid-laden macrophages. Global hemispheric necrosis (Fig. 2.11) is the term used to describe morphologically similar but particularly extensive cases following severe birth asphyxia and sudden hyperpyrexia and collapse in the postnatal period. 2.11 Global hemispheric necrosis. Hemorrhage is the commonest pathology in fetal and neonatal brains. It can start in any intracranial compartment and rapidly spread elsewhere. The pathogenesis is multifactorial. The principal risk factors are immaturity, perinatal distress, and asphyxia, though a similar spatial distribution in still and live births also implicates antenatal factors. The variety of hemorrhages in the neonatal brain is shown in Fig. 2.12. SDH is not related to asphyxia, but is closely related to perinatal distress. Excessive compression and distortion of the head during delivery can disrupt the superior cerebral bridging veins that drain into the sagittal sinus, or the veins to the transverse sinus. More rarely, the falx and sagittal sinus or the tentorium (Fig. 2.13) with the straight sinus or great vein of Galen is torn. SAH (Figs 2.14–2.16) may manifest as: 2.15 Well-demarcated subarachnoid hematomas localized over parietal cortex. 2.16 A small localized SAH on the temporal pole as well as extensive basal SAH secondary to hemorrhagic white matter infarction. SPH is often confused with SAH. It is a focal hemorrhage, which is usually temporal, parietal, or cerebellar, and occurs with or without other signs of bleeding. It is most common in asphyxiated premature infants, but also occurs in premature or term infants with respiratory distress syndrome or congenital heart disease (Figs 2.17, 2.18). 2.17 SPH in a term infant with multiple congenital anomalies including cyanotic congenital heart disease. MACROSCOPIC AND MICROSCOPIC APPEARANCES Acute SEH has variable appearances: small, multiple, and bilateral bleeds occur anywhere in periventricular matrix tissue (Fig. 2.19), including the roof of the fourth ventricle. Acute SEH is usually found 2.19 SEH in an infant with hypoplastic left heart syndrome born by cesarean section at 36 weeks’ gestation who survived 3 days.
Fetal and neonatal hypoxic–ischemic lesions
 The extraordinarily rapid growth and plasticity of the immature nervous system.
The extraordinarily rapid growth and plasticity of the immature nervous system.
 The major changes in cell and tissue properties that occur during development.
The major changes in cell and tissue properties that occur during development.
 PATHOGENESIS OF HYPOXIC–ISCHEMIC LESIONS
PATHOGENESIS OF HYPOXIC–ISCHEMIC LESIONS
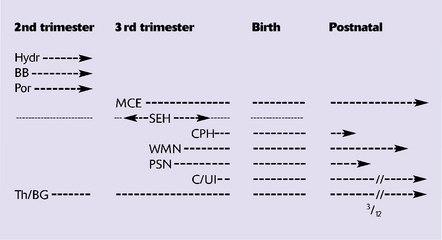
Hydr, hydranencephaly; BB, basket brain; Por, porencephaly; MCE, multicystic encephalopathy; SEH, subependymal hemorrhage; CPH, choroid plexus hemorrhage; WMN (PVL), white matter necrosis (periventricular leukomalacia); PSN, pontosubicular necrosis; C/UI, cortical necrosis/ulegyria; Th/BG, thalamus/basal ganglia damage.
FETAL LESIONS
 CAUSES OF HYPOXIC–ISCHEMIC LESIONS
CAUSES OF HYPOXIC–ISCHEMIC LESIONS
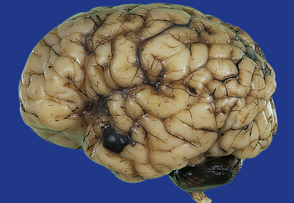
HYDRANENCEPHALY

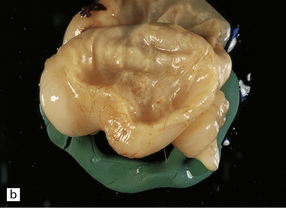
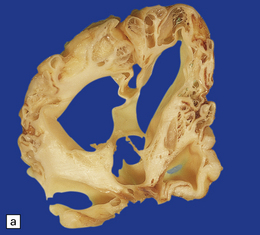
(a) The bubble-like hemispheres photographed under water and viewed from above. (b) Removal from water allows the diaphanous membrane of the cyst wall to collapse. Damage is largely restricted to the internal carotid artery territory with sparing of the orbitofrontal cortex and inferior temporal and occipital lobes.
BASKET BRAIN
 ETIOLOGY AND PATHOGENESIS OF FETAL HYPOXIC–ISCHEMIC LESIONS
ETIOLOGY AND PATHOGENESIS OF FETAL HYPOXIC–ISCHEMIC LESIONS
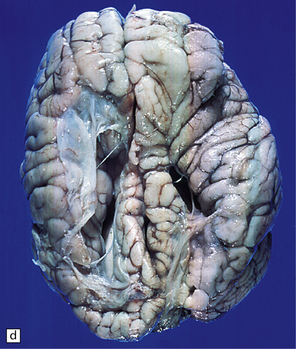
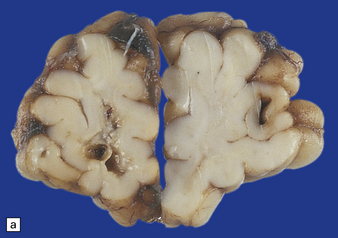
PORENCEPHALY AND SCHIZENCEPHALY
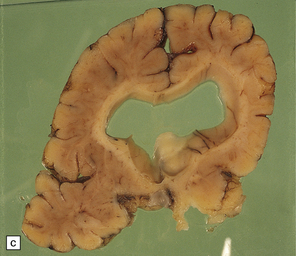
(a) Two unilateral pori are present. The shallow depression in the orbitofrontal cortex contrasts with the wide-mouthed full-thickness defect in the occipital lobe allowing communication between the subarachnoid space and the ventricle. (b) The surrounding convolutions have a radiating pattern. (c) Coronal section through the frontal lobes showing the extent of the anterior defect, which is lined by nodules of gray matter. The septum pellucidum is absent.
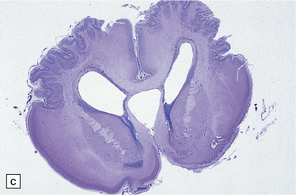
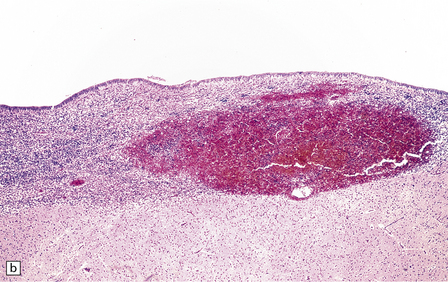
Coronal section through a frontal porus in a 48-year-old man. The cortical gray matter dips down into the cleft to meet the white gliotic ependyma. The cortical ribbon around the edge of the defect is irregularly thickened and disorganized. (Courtesy of Dr T Moss, Frenchay Hospital, Bristol.)
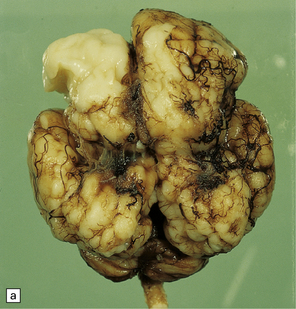
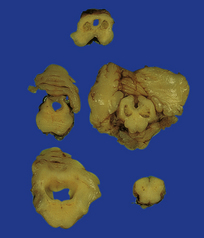
(a) Bilateral porencephalic clefts centered on the middle cerebral artery territory in a twin of 32 weeks’ gestation whose co-twin died at 19 weeks. The hemispheres are viewed from above. (b) Coronal section at anterior thalamic level. The cortex in the center of the lesion is a completely disorganized mixture of neuroblasts and macrophages surrounded either side by polymicrogyric cortex. (c) Coronal section at striatal level. Polymicrogyric cortex from the anterior border of the cleft. (d) Large bilateral full-thickness defects in a 4-year-old boy with cerebral palsy and epilepsy. The covering leptomeninges ruptured during the dissection, revealing a radial pattern of convolutions around the clefts. (e) Coronal sections through the posterior parts of the hemispheres show thick polymicrogyric cortex curling over the mouths of the clefts and deeply invaginating the ventricle. Note the heterotopic gray nodules in the inferior corners of the ventricles.
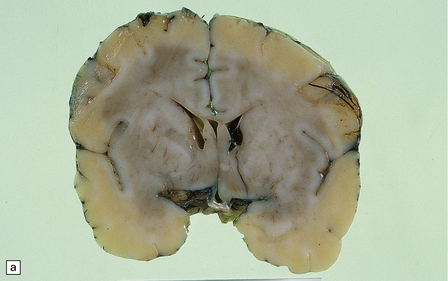
MULTICYSTIC ENCEPHALOPATHY
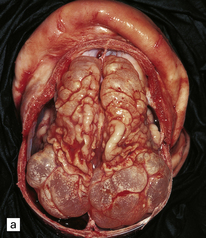
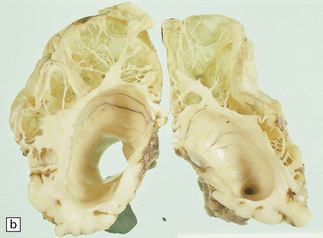
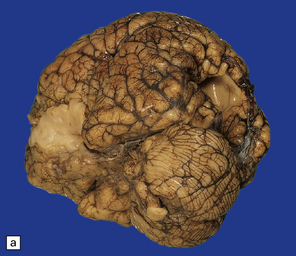
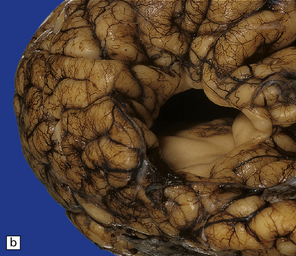
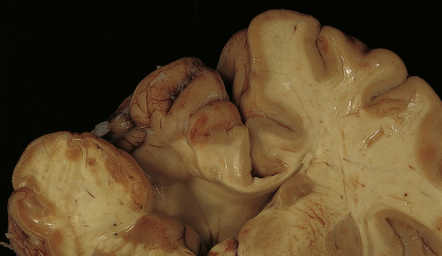
(a) Superior view of the brain within the skull. The convolutions are either massively cystically dilated or narrow and thin. (b) Coronal section showing dilated ventricles and replacement of much of the cortex and white matter by an irregular firm white cystic meshwork.
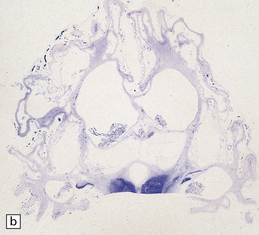
(a) Tough gliovascular bands transform much of the deep cortex, white matter, and basal ganglia into a spongy mass. The thalamic nuclei are shrunken and extremely white. (b) Comparable histologic section from another patient showing that not only the cortex and white matter, but also the thalami and basal ganglia have been replaced by large cysts.

Destruction is limited to the occipital lobe in one of a pair of conjoined twins.
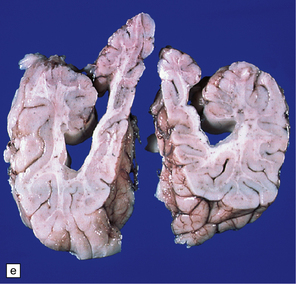
MICROSCOPIC APPEARANCES

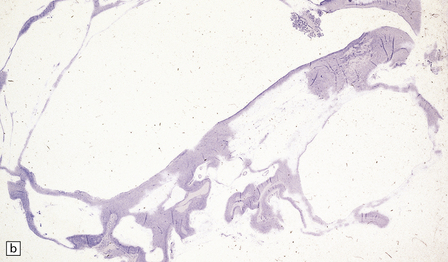
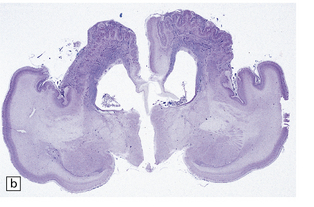
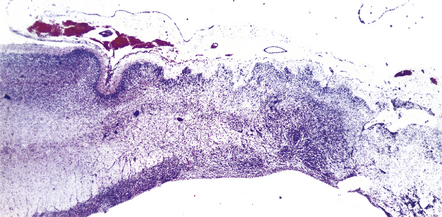
(a) Extensive cystic destruction of the cortical white matter and basal ganglia following severe birth asphyxia. (Courtesy of Dr T Moss, Frenchay Hospital, Bristol.) (b) Low-power section of the frontal lobe.
PERINATAL LESIONS
SUBDURAL HEMORRHAGE (SDH)
SUBARACHNOID HEMORRHAGE (SAH)

This was associated with a threatened abortion at 20 weeks’ gestation.
This occurred in a term infant with multiple congenital anomalies who was cyanosed at birth.
 Petechial or diffuse extravasates.
Petechial or diffuse extravasates.
 Massive localized temporal or occipital hematomas.
Massive localized temporal or occipital hematomas.
 Hemmorhage in the basal cisterns and cerebellar subarachnoid spaces.
Hemmorhage in the basal cisterns and cerebellar subarachnoid spaces.
SUBPIAL HEMORRHAGE (SPH)
(a) Anterior coronal sections in the frontal lobes showing right-sided central white matter softening and several superficial hemorrhages. (b) Microscopy reveals an entirely intracortical bleed covered by pia.
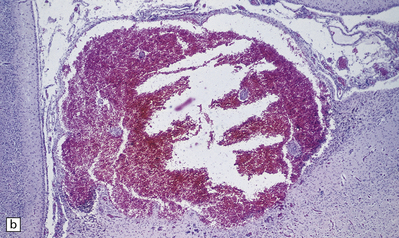
SUBEPENDYMAL GERMINAL PLATE/MATRIX HEMORRHAGE (SEH)
(a) Small SEH that has remained within the matrix zone (grade 1) in the most typical position near the terminal vein close to the caudate nucleus and thalamus. (b) The small bleed remains in situ within the cellular matrix tissue. The ependyma is intact. No bleeding point can be ascertained.
 GRADING OF SEH ON CRANIAL ULTRASOUND
GRADING OF SEH ON CRANIAL ULTRASOUND
Grade
Distribution of hemorrhage
1
Confined to germinal matrix
2
Germinal matrix and lateral ventricle, but no ventricular dilatation
3
Germinal matrix and lateral ventricle, which is acutely distended by hematoma within the ventricle
4
As above with extension of hemorrhage into adjacent brain parenchyma. (Note: the appearances may resemble those of pure venous infarction without IVH; see Fig. 2.36)
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Fetal and neonatal hypoxic–ischemic lesions




























 HYDRANENCEPHALY
HYDRANENCEPHALY


 CLINICAL DIAGNOSIS OF PERINATAL ASPHYXIA
CLINICAL DIAGNOSIS OF PERINATAL ASPHYXIA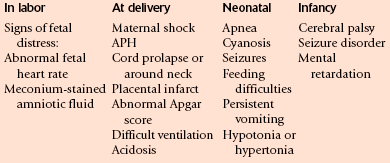
 PORENCEPHALY
PORENCEPHALY


 MULTICYSTIC ENCEPHALOPATHY
MULTICYSTIC ENCEPHALOPATHY