SECTION I GENERAL APPROACH TO HISTORY AND EXAMINATION
NERVOUS SYSTEM – EXAMINATION
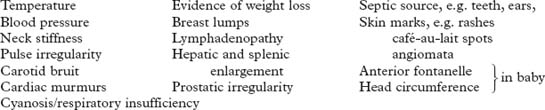
Neurological disease may produce systemic signs and systemic disease may affect the nervous system. A complete general examination must therefore accompany that of the central nervous system. In particular, note the following
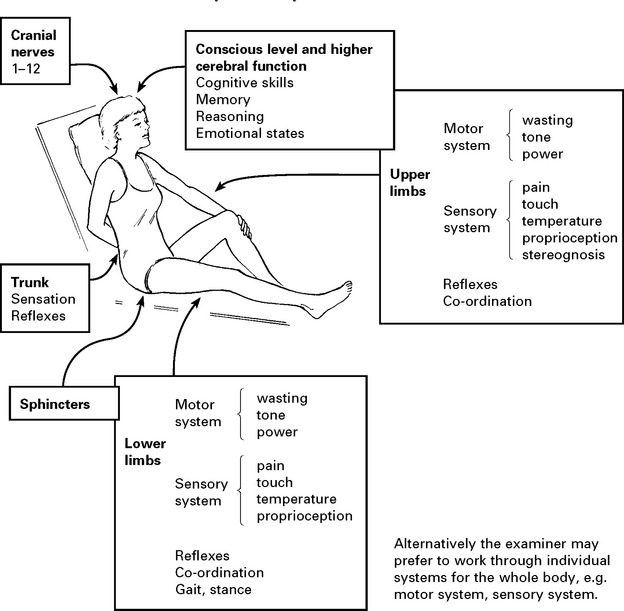
CNS examination is described systematically from the head downwards and includes:
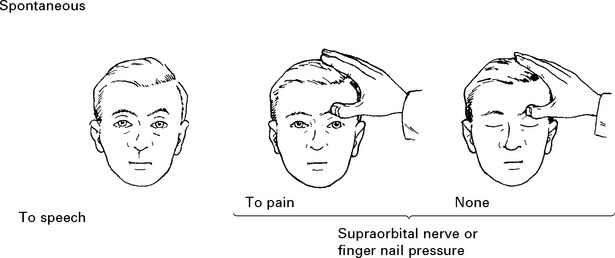
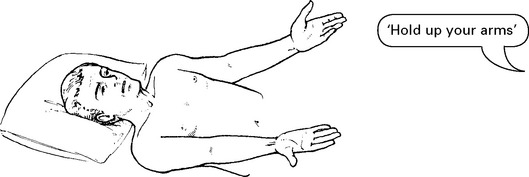
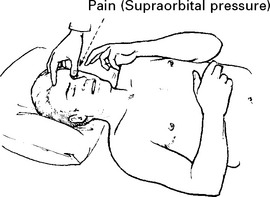
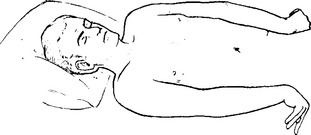
EXAMINATION – CONSCIOUS LEVEL ASSESSMENT

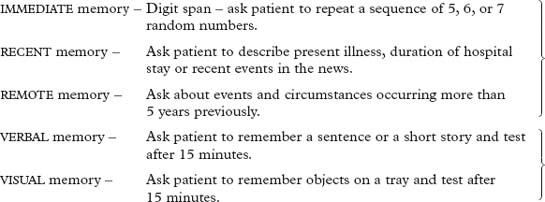
EXAMINATION – HIGHER CEREBRAL FUNCTION
COGNITIVE SKILL
Dominant hemisphere disorders
| Listen to language pattern | Expressive dysphasia | |
| Receptive dysphasia | ||
| Does the patient understand simple/complex spoken commands? e.g. ‘Hold up both arms, touch the right ear with the left fifth finger.’ | Receptive dysphasia | |
| Ask the patient to name objects. | Nominal dysphasia | |
| Does the patient read correctly? | Dyslexia | |
| Does the patient write correctly? | Dysgraphia | |
| Ask the patient to perform a numerical calculation, e.g. serial 7 test, where 7 is subtracted serially from 100. | Dyscalculia | |
| Can the patient recognise objects? e.g. ask patient to select an object from a group. | Agnosia | |
Non-dominant hemisphere disorders
| Note patient’s ability to find his way around the ward or his home. | Geographical agnosia |
| Can the patient dress himself? | Dressing apraxia |
| Note the patient’s ability to copy a geometric pattern, e.g. ask patient to form a star with matches or copy a drawing of a cube. | Constructional apraxia |
Mini Mental Status Examination (MMSE) is used in the assessment of DEMENTIA (page 127).
REASONING AND PROBLEM SOLVING
Ask patient to reverse 3 or 4 random numbers.
Ask patient to explain proverbs.
Ask patient to sort playing cards into suits.
CRANIAL NERVE EXAMINATION

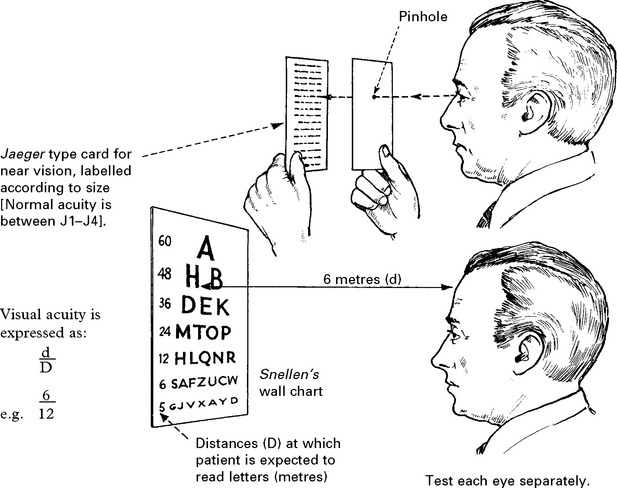
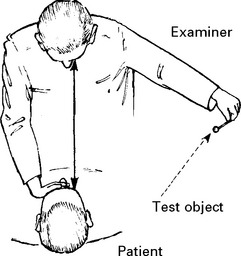
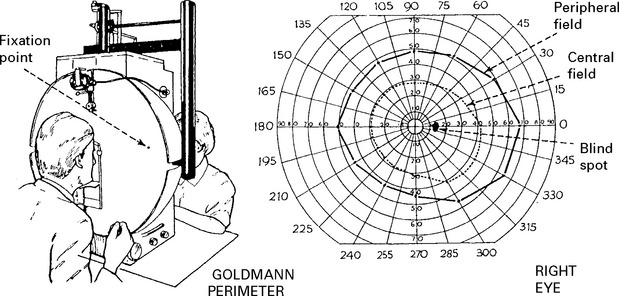
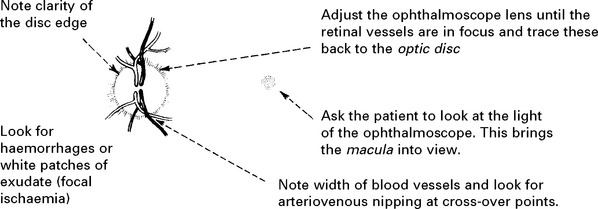
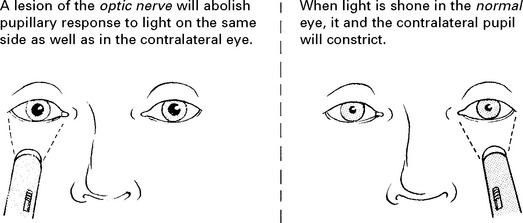
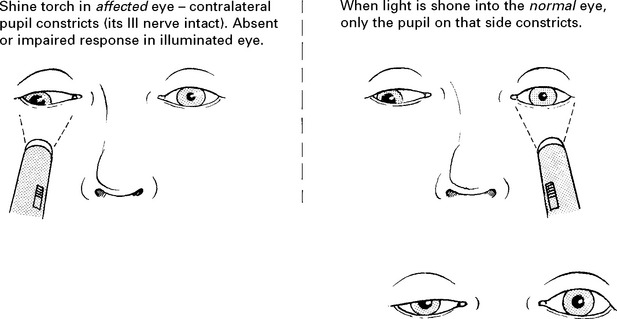
OPTIC NERVE (II)

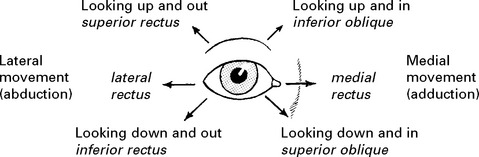
OCULOMOTOR (III), TROCHLEAR (IV) AND ABDUCENS (VI) NERVES
Pupil: The pupil dilates and becomes ‘fixed’ to light.
Ocular movement

Note any malalignment or limitation of range.
Question patient about diplopia; the patient is more likely to notice this before the examiner can detect impairment of eye movement. If present:
Related posts:
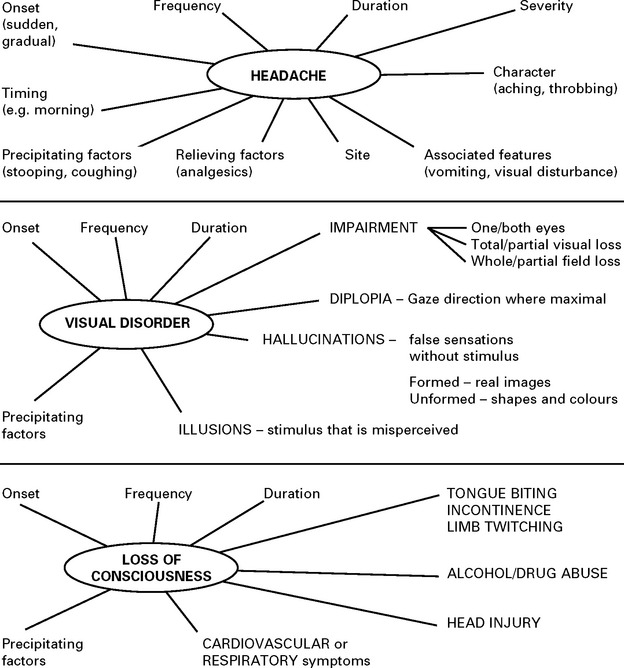
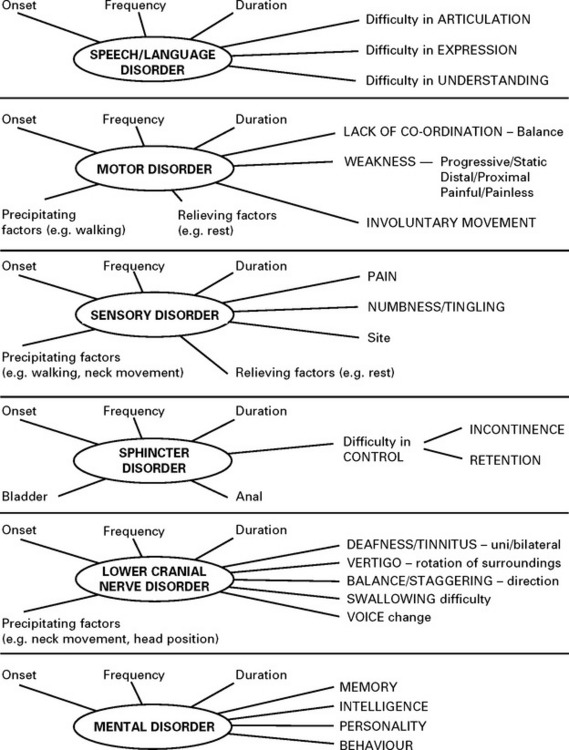
 CLINICAL PRESENTATION, ANATOMICAL CONCEPTS AND DIAGNOSTIC APPROACH
CLINICAL PRESENTATION, ANATOMICAL CONCEPTS AND DIAGNOSTIC APPROACH
 LOCALISED NEUROLOGICAL DISEASE AND ITS MANAGEMENT C. PERIPHERAL NERVE AND MUSCLE
LOCALISED NEUROLOGICAL DISEASE AND ITS MANAGEMENT C. PERIPHERAL NERVE AND MUSCLE
 LOCALISED NEUROLOGICAL DISEASE AND ITS MANAGEMENT B. SPINAL CORD AND ROOTS
LOCALISED NEUROLOGICAL DISEASE AND ITS MANAGEMENT B. SPINAL CORD AND ROOTS
 INVESTIGATIONS OF THE CENTRAL AND PERIPHERAL NERVOUS SYSTEMS
INVESTIGATIONS OF THE CENTRAL AND PERIPHERAL NERVOUS SYSTEMS
 LOCALISED NEUROLOGICAL DISEASE AND ITS MANAGEMENT A. INTRACRANIAL
LOCALISED NEUROLOGICAL DISEASE AND ITS MANAGEMENT A. INTRACRANIAL
 MULTIFOCAL NEUROLOGICAL DISEASE AND ITS MANAGEMENT
MULTIFOCAL NEUROLOGICAL DISEASE AND ITS MANAGEMENT
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


