After a century of development, group therapy is today one of the most widely practised treatment methods in psychiatry with an extensive literature. There are three principles common to its wide range of applications. First, the therapist calls the ‘community’ into the consulting room where, together with the therapist, it becomes the therapeutic agent. Second, the therapist assembles a group of people who can contribute to a commonly held resource from which its members can each derive benefits. And third, the therapist does nothing for them in the context of the group, that they can do for themselves, and one another.
This chapter starts by providing a conceptual framework that differentiates methods, models, and applications for the practice of group therapy in adult psychiatry. After classification of the different methods and applications we discuss the main theoretical models; explore the dynamic life of therapy groups; consider some of the key clinical issues facing practitioners; their applications to a range of patient populations and settings; their evaluation and justification and their historical evolution this century. In the conclusion we consider the planning of group services and the training of their practitioners. This revision of the chapter has brought it up-to-date with the contemporary literature in a field that has seen a great deal of innovation since the original 2000 edition.
The developing evidence base for group psychotherapy is ‘Guardedly optimistic. The literature has become stronger and deeper and is capable of supporting evidence-based treatment recommendations for some patient populations.’ The evidence base for the effectiveness of group psychotherapy has been growing with the field. Some 700 studies, spanning the past three decades, have shown that the group format consistently produced positive effects with diverse disorders and treatment models.(1) These show that both individual and group psychotherapy will effect much the same set of results. For group therapy to be effective it has to utilize those therapeutic factors originally laid out by Foulkes(2) and later by Yalom(3)—the group has to be the primary focus of therapy; patients need to be well selected; and therapists need to be adequately trained. The chapter will address these questions of focus, selection, and training.
Although the two authors of this chapter are both group analysts, we have set out to provide a full account of the wide range of group work practice. The United Kingdom is our own working location which lends emphasis to the chapter but it is compiled with sources and references that address the international field and it gives attention to current literature in many countries including North and South America and Continental Europe.
Basic methods
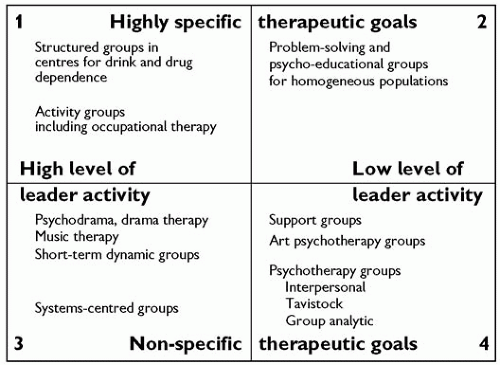
In Fig. 6.3.6.1 we have used two simple factors—therapeutic goals and group leadership—to provide a simple classification of the many different methods.
Therapeutic goals
Groups will be more or less specific in their therapeutic goals. For example, those catering for a homogeneous population with a commonly defined problem whose solution provides the basis for entry to the group—such as overcoming drink or drug dependence—are classified here with specific goals. Groups that provide psychoanalytic psychotherapy, whether run according to Interpersonal, Tavistock, or Group-Analytic models, are classified here with nonspecific goals. There is a wide range of variation between these extremes and within each of these main psychodynamic models.
Leadership
The more the leader directs the group, the more prominent he becomes as the group’s ‘model object’. The less the leader directs the group, the more scope there is for the emergence of unconscious dynamics and for attention to transference and counter-transference. In this case, therapy progresses through the development of relationships. The greater the leadership activity, the more likely it is that group members are being offered a technique or skill in the setting of a group. The lower this activity, the stronger will be the relational content of the therapy and the therapist’s skills of fostering relationships will equip the group to work developmentally and in depth on both the obvious and hidden issues that its members bring. The three principal psychodynamic methods discussed in The principal model of psychodynamic group therapy below share a non-directive philosophy with subtle but significant differences between their models of practice.
Fig. 6.3.6.1 A simple classification of group methods.
Using these two basic indicators—specificity of goals and levels of leadership activity—the four quadrants in the diagram provide us with a simple way of ‘placing’ the different group therapies.
Goal-specific therapy with high level of leader activity: quadrant 1
In many drug and alcohol dependency regimes, participants are required to fulfil obligations tied to each stage of a structured programme. They move forward when stage-specific obligations are fulfilled. As the novice moves up, he/she becomes a trainer to the newcomers with the therapist(s) directing the process in active terms. Cognitive therapy given in a group setting uses the group as an assembly who learn from and discuss with the expert. Dependency on a shared and valued leader, and attention to group dynamics amplify the learning and some group cohesion develops, but this is not the primary focus of the therapy.
Goal-directed with lower level of leader activity: quadrant 2
Problem-solving or psycho-educational groups for homogeneous populations, such as those set up for eating disorders or offenders, which are run along analytic lines, can be placed in this category. Although there are clear and directed goals, the leader’s level of activity is confined to a facilitating, linking, or enabling one, followed by analysis and interpretation. Group discussion and cohesion amplify the affective experience and enhance the learning.
Non-specific goals with high level of leader activity: quadrant 3
In psychodrama groups, leadership is explicitly vested in the psychodrama director. The needs and goals of group members are diffuse and often diverse and, in psychiatric practice, will have to do with relief from mental suffering. The psychodrama director can draw on many techniques. Affective arousal can be high so the power of sharing through discussion and the sympathy; and empathy of group members towards one another become powerful therapeutic tools. Strong conflict arousal and its subsequent resolution is similarly therapeutic.
Systems-centred therapy (as developed by Agazarian)(4) similarly provides a high level of leadership activity for groups that have non-specific goals. Short-term dynamic groups are frequently constituted with non-specific goals but are run over 10 or 20 sessions by leaders who maintain a high level of involvement and direction, often demarcated according to the different stages of the group’s progress.
Non-specific goals with low level of leader activity: quadrant 4
The goals of group-analytic or psychoanalytic group therapy are most frequently diffuse and non-specific involving relief from symptoms and other forms of suffering; personal growth; and psychological change. There are three main schools considered in this chapter—the Interpersonal (Yalom), Tavistock (Bion or groupas-a-whole), and the Group-Analytic. They share non-specific goals and have low levels of leader activity but differ from one another in how the leadership role and function is understood and discharged. They share assumptions about the importance of unconscious individual and group dynamics and look to the group for its transformational potential. Their differences affect the way in which transference and counter-transference is understood and worked with. There is a comparative appraisal of these models below.
The application of basic methods
We now provide a more detailed overview of the current field and offer a brief set of training requirements for practitioners in each of the methods discussed.
The field can be divided into five basic methods—activity, supportive, problem-solving, psycho-educational, and psychodynamic. The first three methods are goal-specific as indicated by their descriptions, the fourth is less specific and the fifth is a nondirective analytic psychotherapy. In supportive and problem-solving groups, therapeutic leadership can be highly directed or not, depending on the approach. Activity and psycho-educational groups will inevitably have a high level of directed group leadership, whilst psychodynamic groups have a much lower level of directed group leadership. All five methods rely on the same basic procedures—the selection and grouping of a number of people seeking help who have regular meetings together with one or more well-trained therapist(s).
Activity groups
The most vulnerable and disturbed patients can be placed in therapy groups defined by an activity that provides a convening function such as exercise or cooking. They can then be used to create conditions for a wide range of secondary functions that foster affiliations, develop social skills, address unspoken anxieties, and express troubling emotions. Occupational therapists and nurses using art media or other socially syntonic activity like gardening or hair-dressing have been developing a wide range of group services in both acute and rehabilitation psychiatry for many years.(5) The approach has been used in a wide range of other settings including medical rehabilitation, rehabilitation with refugees, social work and fostering, and adoption programmes. Groups that keep the original activity as their primary focus, working with art media for example, need to be differentiated from those which use such media to develop an analytic focus on psychological work. The arts psychotherapies belong to this latter group. They have non-specific therapeutic goals and might, as in the case of music therapy, have a high level of leadership activity or, in the case of art therapy, have a low level of leadership activity.
Whilst therapists do not engage in the uncovering and exploration of unconscious dynamics, they will need leadership abilities, capabilities in organizing group activities, and should have a basic understanding of psychopathology and group dynamics.
Supportive groups
These groups function as a form of social support providing containment, the improvement of social skills, and the enhancement of participants’ capacities for social adaptation. They aim to reduce the deleterious effects of social isolation, bring people out of withdrawal into a social context, and provide opportunities for problem sharing. They cater to patient populations with long-standing personality disorders not open to uncovering exploration; those with chronic mental and physical illness,(6) physical handicap, mental retardation, and carers for those with any of these problems. They will often allow a certain amount of psychoeducation with the group leader influencing members’ attitudes as in the case, for example, of a group for young sexually active adults with learning disability who might receive guidance on contraception.
Whilst therapists do not engage in the uncovering and exploration of unconscious dynamics, they will need leadership abilities, capabilities in organizing group activities, and should have a basic understanding of psychopathology and group dynamics.
Problem-solving groups
Group therapy is provided for a set of referral criteria to resolve a defined and sometimes circumscribed problem. Alcoholics Anonymous, Alanon, Gamblers Anonymous, and groups for people with poor impulse control, eating disorders, or other habitual problems such as smoking, are a few of the examples. These groups can take on many of the features of long-term support groups, in that they offer ego-supportive and adaptive resources, providing an extended service for monitoring by the patient or by professionals, without necessarily committing members to the deeper and more radical analytic work entailed by a psychodynamic group. In many cases, the problem-solving focus provides a convening frame by which to engage a population who are soon drawn into psychodynamic work that sees them through profound changes. Many of the groups run by clinicians in primary hospital care—occupational therapists, nurses, doctors, and psychologists—take this form. The Group Work Programme at the Medical Foundation For Victims Of Torture in London is another example (see also section on trauma in specical population, below).
Where they cater for the more severely disturbed, staff will need to be well-trained in one of the core professions. They will need leadership abilities, capabilities in organizing group activities, should have a basic understanding of psychopathology, and be sufficiently well-trained to explore the dynamic group issues that lead from the problem back to the personality structure of their membership. If therapeutic goals involve major changes in personality and social functioning, this will involve the uncovering and exploration of unconscious dynamics.
Psycho-educational groups
The original groups for servicemen with war neurosis at Northfield took this form in which people were given the role of students of their disorders rather than ‘sick’ people. Patients become open to new information and are better able to unlearn maladaptive attitudes about the nature of their disorder. This more cognitive approach can be applied in homogeneous problem-solving groups. Information can be provided through lectures, discussions, and suitable reading material. There are different ways of lowering anxiety and uncovering maladaptive and inappropriate attitudes towards such problems as anxiety states, phobias and obsessions, and psychosomatic disorders. Many of the groups run for those with serious physical illness (see also section on the medically ill in special populations, below) take this form. And there is often a major psycho-educational component in support groups—for example, those with chronic mental illness who can be helped to understand and cope with delusions, hallucinations, and the stigma of illness.(7) (see also section on the mentally ill in special populations, below)
Staff need leadership abilities; capabilities in organizing group activities, a basic understanding of psychopathology, and need to be sufficiently well-trained in their chosen problem area to be able to relate its educational focus to thematic group issues. If therapeutic goals involve major changes in personality and social functioning, this will involve the uncovering and exploration of unconscious dynamics.
Psychodynamic groups
There are supportive, problem-solving, and psycho-educational components in all psychodynamic groups, but the description ‘psychodynamic’ is reserved for those in which the declared goal is lasting personal change through a non-directive, free-associative therapy. The range of different group contexts is so varied that—at first sight—they might appear to have little in common. But there will be common principles offering therapy to a group of people on an in-patient unit recovering from psychosis and meeting thrice weekly; those in a secure unit for violent offenders meeting once weekly; and those—including mental health trainees—attending a group in private practice once or twice weekly. These principles can be summarized in the table, Table 6.3.6.1 below.
Within these parameters therapy is part of the cultural domain of all shared, conversational experience in which people struggle with meaning—in congregational life, in the confessional, in theatre, narrative or poetry.(8,9)
Staff need to be trained to the level already described. They need good leadership ability, capabilities in organizing group activities, and a good understanding of psychopathology. Beyond these requirements, therapeutic goals will involve major changes in personality and social functioning involving the uncovering and exploration of unconscious dynamics. So staff will need access to a range of specialized training opportunities which should provide psychodynamic theory, clinical supervision and, ideally, some opportunity for the practitioners’ own personal development.
Table 6.3.6.1 Organizing principles for group therapy
1
Members will have been chosen by the therapist.
2
They will have chosen to join and participate.
3
They will be expected to justify their place by reliable attendance and participation.
4
The work will be governed by a psychotherapeutic contract.
5
The contract will include definitions of confidentiality and other boundaries.
6
A therapeutic alliance with individual members will be established either prior to their joining the group or during the early stages of their attendance in the group.
7
Agreed parameters will include the duration and time-boundaries of the group as well as its membership and composition.
8
Groups can be homogeneous or heterogeneous.
9
Groups may have a fixed time limit or continue on a slow-open basis for many years.
10
Groups may have a stable and fixed, or a rotating membership with empty places taken by new members.
The contemporary field and its history
The paradigm shift that led to a vision of the group as a whole began over a period of time and in a number of locations. Trigant Burrow coined the term group analysis in the USA in the 1920s.(10,11) Further development in the years after World War II period enabled workers to recognize the dynamics of groups and institutions and led to group and family therapy, milieu therapy, and therapeutic community concept and practice.
Second World War
In Britain and the US, during the Second World War, an appreciation of group psychology led to a wide range of innovations, the most important of which included:
The use of group methods for selection and allocation of work responsibilities
Studies of group morale
The integration of psychiatric knowledge to the management of large groups through the role of the command psychiatrist
The treatment of acute and prolonged battle stress and the rehabilitation of returned prisoners of war.
Clinicians used the opportunities created within army psychiatry to apply methods developed in the pre-war years.(12) Brigadier J.R. Rees, Director of the Tavistock Clinic in the 1930s, largely created this opportunity in the British Army. His Tavistock colleagues formed an ‘invisible college’ and were responsible for signal achievements in the advances in selection and treatment.(13)
Foremost amongst these were Northfield, the military hospital near Birmingham where S.H. Foulkes was a senior medical officer.(14) A refugee from Nazi Germany, Foulkes brought with him from the Frankfurt Institute the revised understanding of Freudian theory that was also to prove influential in the US. In the New School for Social Research, New York, and in the work of Neo-Freudians like Erich Fromm, Frieda Fromm-Reichman, and social theorists like Adorno, Marcuse, and Norbert Elias, psychoanalysis and Marxist theory were brought into a new, creative relationship.(15) In the United Kingdom Foulkes first developed his approach to group therapy in Exeter before the war and was able to apply it successfully on a large scale to the treatment of war neuroses at Northfield.
Post-war period
Group psychotherapy moved from inspirational and didactic models to psychodynamic and analytic ones in the post-war period.
(a) United Kingdom
The Group-Analytic Tradition: Foulkes gathered around him a small group of clinicians and others who developed his ideas and practises. Drawing on the ideas of Trigant Burrow, they called it group analysis and later established the Group-Analytic Society, and trained generations of clinicians. His first book written in the heat of the Northfield experience outlined the basics of his approach.(16) Other publications followed and, with Malcolm Pines, training courses were established which lead to the founding of the Institutes of Group Analysis and Family Therapy, the Association of Family Therapists, and Association of Therapeutic Communities. There are now training courses in group analysis in many centres in the United Kingdom and continental Europe. The Journal, Group Analysis, established by Foulkes, continues to be the major publication in European group psychotherapy. Group-analytic psychotherapy has undergone clinical evaluation by a number of clinicians.(17,18,19)
The ‘Tavistock’ Approach: The approach originates in the work of Bion, Ezriel, Sutherland, and their colleagues. It shares with group analysis an interest in the underlying pattern of object relations in groups but, under the influence of Bion—its major exponent—his ‘basic assumption theory’ is applied to the exclusion of almost everything else. (Bion’s monograph was his only publication on groups and marked the end of his interest in the subject.(20)) The approach has been especially influential in staff training and consultancy which, given the slender theoretical foundations on which it rests, suggests a wide responsiveness in the field of basic assumption theory. The approach has undergone further development in the United States where it is often referred to as group-as-a-whole. When employed as a therapy, it can overlook the individuality of a group’s members, disturbing some patients whose experience of the group situation can repeat early developmental traumas of neglect and misunderstanding by caretakers. Malan’s study of effectiveness(21) raised serious questions about the model’s efficacy in its clinical applications but its training applications continue to influence the field.
(b) United States
(i) Early pioneers
Jacob Moreno was the innovator of group psychodrama, a pioneer form of group psychotherapy.(22) He also introduced sociometry, a scientific method for the study of group affiliations and conflicts, widely accepted and used by social psychologists. Slavson was an educationalist of psychoanalytic persuasion who became the central figure in the early development of group psychotherapy. His clinical influence, particularly with groups for the parents of children in difficulty, and his focus on the dynamics of projection in groups has been of lasting importance.(23) His organizational efforts lead to the formation of the American Group Psychotherapy Association. Emanuel Schwartz began to apply psychoanalytic ideas to group psychotherapy in the late 1930s and was later joined by Alexander Wolf.(24,25) In their approach, people underwent an individual psychotherapy in the setting of a group, a kind of parallel process alongside their fellow patients, with attention focused on the transferential relationship between each individual and their therapist. The approach has been of lasting importance in creating a clinical framework for combining individual and group therapy. Foulkes’ criticism at the time was that the approach overlooked any systematic use of group-specific process. In contrast to their ‘psychotherapy in the group’ he offered group analysis as a clinical alternative, describing it as ‘psychotherapy by the group’.
(ii) Irving Yalom
Yalom’s interpersonal approach is influenced by the interpersonal psychotherapy of Sullivan and Frank. His Theory And Practice of Group Psychotherapy, now in its fifth edition and written jointly with Leszcz, is the first systematic account of groups informed by research and remains one of the most influential books in the field.(3) Yalom’s later text on inpatient group psychotherapy systematized group work in that setting.(26)
(iii) The contemporary field
There are many centres of excellence, a wide range of methods and models and an empirical base grounded in research. The most useful single text is by Rutan and Stone, now in its fourth edition.(27) Collections by Kaplan and Sadock(28) and by Alonso and Swiller(29) cover the field. Psychoanalytic models have a rich diversity of theory with contributions from object relations, self psychology, and social systems theory.(30) The Modern Group movement is amongst the most innovative, beginning with a classic text by Spotnitz(31) and developing through an active training programme, a journal, The Modern Group, and publications by Ormont(32) and others.
(iv) South America
There is a vigorous field of development throughout South America that draws on both the Tavistock and Group Analytic traditions but is informed by independent sources based largely on the work of Pichon-Riviere. Tubert-Oklander and Hernandez de Tubert have introduced this approach, referred to as Operative Groups, to the English-speaking world.(33)
(v) Continental Europe
Group methods have played an active part in the reconstruction of mental health services throughout Europe in the post-war period. Distinctive approaches are emerging. Those in Germany include psychosomatic practice(34) and the Gottingen model.(35) The journal of the Heidelberg Institute of Group Analysis gives access to a vigorous field. A major research study is in process, based in Germany, in which therapists throughout Europe are taking part and which aims to provide a detailed evaluation of group therapy, its patients, and its therapists.(36) Other distinctive developments include those in Italy(43) and original training models, for example, those in Greece(37) and Norway.(38)
Principal models of psychodynamic group therapy
The therapist
The therapist is responsible to the group— and to the institution in which it is set—for achieving and maintaining professional competence and should have a level of training appropriate to the task. A formal qualification in psychotherapy is the ideal training. This will have included theory, personal therapy for the therapist, and clinical supervision. Mental health professionals from all disciplines make an active contribution to a rich and diverse service with the training requirements of theory and supervision arranged at their workplace. The opportunity to run a group is provided in most psychiatric and psychology training programmes. Many centres and training institutions offer training in group methods and several are wholly committed to the training of group therapists who have their own professional associations in the UK and internationally. Private once- or twice-weekly analytic groups are now regarded by many mental health professionals as the therapy of choice for their personal development. Other requirements for a good therapist are listed in table 6.3.6.2.
(a) Making a beginning
The establishment of a group begins as a management task in the definition of its goals, recruitment of its members, protection of its setting, venue and timetable, and in the maintenance of its ongoing life. It evolves as a therapeutic task in which the therapist is responsible for maintaining a therapeutic attitude to the individual members and to the group as a whole. Powerful affects and attitudes will be directed towards her which she will monitor and transform into verbal and non-verbal therapeutic responses.
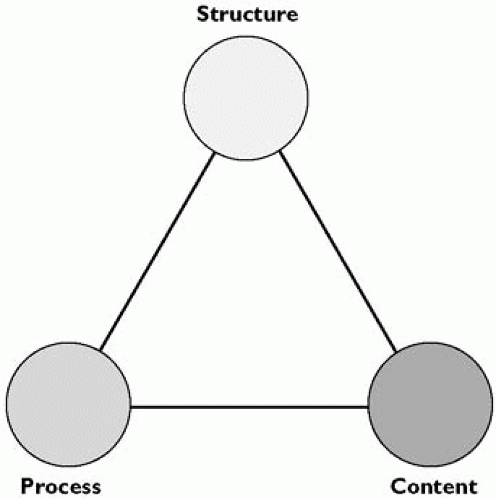
The therapeutic rationale will allow the therapist to be discriminating and consistent about interventions of various kinds during the life of the group and what follows below provides an orientation— based on the dynamic elements of structure, process and content— to the three main models used in the UK.
Structure, process, and content: the dynamic elements of a group
Regardless of the therapist’s method, people usually start in groups with a form of serial monologue. Out of this arise the capacities to talk and listen that are often undeveloped or even non-existent at the outset of therapy but which are its core constituents. From talking and listening comes self-disclosure and out of this social exchange identification emerges, which in due course leads to dialogue and differentiation. So the conductor must give a place to monologue whilst, at the same time, cultivating dialogue—the exchange between members or sub-groups—and, ultimately, promoting discourse, defined here as the free interaction of participants in the flexible and complex exchange that distinguishes the communication of a group.
Table 6.3.6.2 Requirements for therapeutic competence
Requirements for therapeutic competence include:
1
The ability to follow complex interactions and processes.
2
The ability to discriminate between appropriate activity and a containing form of silence.
3
A reflective attitude and the capacity to consider and reflect upon the processes concerning both the individual members and the group as a whole.
4
An eye for both the visible and invisible group and a curiosity about the unconscious or otherwise hidden aspects of a group’s life. This will require the therapist’s access to their own internal process and a capacity to make use of it.
5
A therapeutic rationale for action related to the group tasks and leadership requirements including the psychopathology of the individuals, their psychodynamics, and group dynamics.
Structure describes the more enduring aspects of any group’s makeup, the ‘architecture’ of its interpersonal relations conceptualized first in terms of the setting and its boundaries and then conceptualized in the bond between each individual, the therapist(s), and the group as a whole. Process describes the fluid and dynamic fluctuations of emotion and experience, the business of relating and communicating, the changes of association and inter-member responses. The content of a group’s exchange is in its visible and audible events, in the narrative line and dramatic content of peoples’ encounters, the topics raised, their thematic development, and the extent to which they are explored or avoided.
As Fig. 6.3.6.2 illustrates, each of these three dynamic elements has a determining influence on each of the others. For example, a group in which there was a problem caused by the institution’s failure to honour its commitment to reliable space for regular meetings, would have a serious structural problem. Intrusion, relocation, or a conflict over space might then emerge in the content of the members’ associations as they talked about shared past experience. The therapist would need to decide whether to direct the process towards the connection between past and present anxieties, or reassurance that the therapist would—from now on—be able to protect their space.
(a) Overview of the Interpersonal, Tavistock, and Group-Analytic Models
In the Interpersonal school, intra-group interactions, including those between its members and the leader, are taken in their totality, but differentiating the leader as a different ‘sort’ of person from the others. In the Tavistock model, a two-body psychology is used to analyse the interchange between the leader and the group taken as a whole. The therapist’s principal role is in the analysis and interpretation of defences against primitive anxieties (or basic assumptions). The Group-Analytic Model calls on elements of both foregoing models. Like the Tavistock model it considers the leader as structurally different to other group members but like the Interpersonal model, it encourages the leader to work in the group with individuals. A three-body psychology is used to understand the role of the leader who is referred to here as the conductor. Therapy proceeds through the dynamic interaction between each individual, the conductor, and the group as a whole.
Fig. 6.3.6.2 The dynamic elements of a group.
(b) The model of interpersonal group therapy
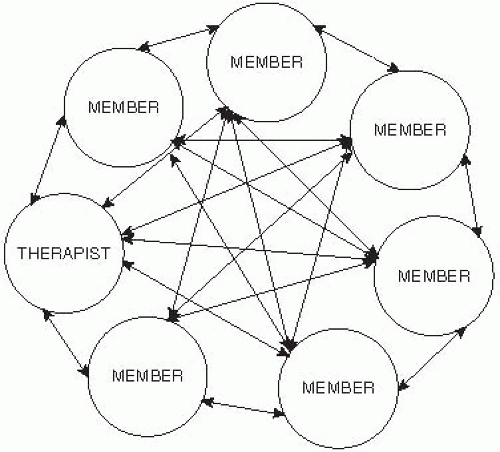
The focus is on interpersonal learning as a primary mechanism of change. The group provides the antidote to maladaptive interpersonal beliefs and behaviours through feedback from others and encouragement to experiment with healthier behaviours first within the group and then outside. The joint examination of intra-group transference reactions allows members to replace processes that have a historical origin in the ‘there and then’, the dynamic past, with those more appropriate to the ‘here and now’, the dynamic present. The approach emphasizes the educational opportunities of working in the ‘here and now’ of the group. The therapist takes the responsibility for leading the group towards awareness of these interpersonal dynamics and their expressions. There is also greater therapist transparency than in other psychodynamic approaches with the therapist modelling desired behaviours, sharing the reactions to events in the group directly, and being open to feedback from other group members.
As the diagram indicates, interpersonal dynamics are kept at the forefront of members’ attention by the therapist. This sets a pattern in which the content of members’ discussions and the process of their interactions gives the group its agenda. The interpersonal approach places the therapist amongst other members of the group without giving him a distinctive structural identity and omits any formal demarcation for the boundaries of the group as a whole.
The model provided the early descriptive research on the phases of small groups, on the basis of which Yalom tabulated the curative factors in a group’s life (see Table 6.3.6.3).
This construction has been very influential. Yalom’s use of the term ‘curative’ poses many problems for those clinicians who see the goals of therapy involving personal growth and change. He did much to address this difficulty by singling out the last of his ‘curative’ factors—existential issues—for special treatment in a subsequent text.(49)
(c) The Tavistock model
Bion’s ideas have an explanatory power and simplicity of application that continues to prove illuminating.(40) In a group at any point in time, its culture and climate are governed by primitive, unconscious anxieties that impede its capacities for rational work in which the person or representation of the leader plays a crucial part. The anxieties, organized into one of three categories, referred to as basic assumptions, are dependency, fight or flight, and pairing. They affect the group as a whole in which only one basic assumption is believed to be operative at any point in time. Bion saw basic assumptions as interfering with the ‘work group’, the more rational, higher-level functioning of the group and its members. The therapist’s key task lies in understanding and interpreting the operative basic assumption to the whole group. The meaning of individuals’ experience is subsumed by this understanding of the whole. This therapist-centred approach sees transference only as directed towards the therapist who represents authority. In dependency, the group tries to elicit protection through passive or dependent behaviour. In fight/flight they will attack the therapist or some other issue; or retreat and withdraw. And in pairing they may create a group illusion that some magical form of rescue may arise from the dilemmas of group life through charged partnerships. Hopper has introduced a fourth basic assumption that he calls massification/aggregation in which the defensive structures of groups or societies in crisis is thought to entail either a rigid fusion of identities excluding individuality, or extensive withdrawal preventing mutuality.
Fig. 6.3.6.3 The elements of an interpersonal group.
Table 6.3.6.3 Yalom’s curative factors
1
Instillation of hope
2
Universality
3
Imparting information
4
Altruism
5
Corrective recapitulation of primary family group
6
Development of socializing techniques
7
Imitative behaviour
8
Interpersonal learning
9
Group cohesiveness
10
Catharsis
11
Existential factors
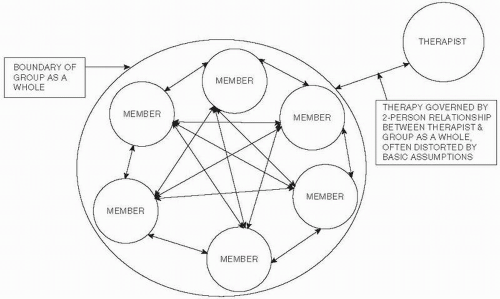
Fig. 6.3.6.4 The elements of a Tavistock group.
The two-body psychology used here enforces a series of clinical constraints that reduce the complexity of group interaction to a bi-personal exchange between therapist and group taken as a whole. As Fig. 6.3.6.4 illustrates, intra-group dynamics are considered only in their entirety for what they reveal about the unconscious state of the group as a whole, and for what they indicate about the nature of the group’s relationship with the therapist. Figure 6.3.6.4 illustrates how the therapist stands outside the group in a stance that is not only neutral and dispassionate but also opaque and withholding of self.
Ezriel, basing his work on Bion, developed his theory of common group tension.(41) He believed that the group would be caught up at any given time in a commonly shared conflict centred on the unconscious fear of catastrophe, what he called the dreaded state. People would avoid a state in the group—say one in which they talked about sad feelings—because of the unconscious fear that talking about sadness would lead to a dreaded state, in this case a depressive collapse. A group would be driven into unconscious, defensive organization—what he called the required state—to keep sadness at bay. For example, an extended period of manic humour, the required state, would help prevent the avoided state, sadness, and this would in turn protect against the dreaded state. Interpretations would allow members to become increasingly aware of the underlying catastrophic fears and reduce their need for defensive organization.
Horwitz calls Ezriel’s approach ‘deductive’, in that it relates individual’s contributions only to the common group tension. He realized that this deductive approach was clinically unproductive and developed, what he called an ‘inductive’ method which is group-centred.(42) Interventions are first addressed to individual members in the group. Only after working with patients individually does the therapist introduce a common theme that binds them together. Thus the therapist, as in the Group-Analytic model, works on a figure/ground basis in which individual contributions are valued and explored in their own right before they are contextualized in the life of the group as a whole.
Another approach, focal conflict theory, as developed by Whitaker and Lieberman(43) is similar to Ezriel’s in focussing the therapist on a conflict that becomes his point of emphasis, but it answers Horwitz’s criticisms. On their account, underlying disturbing motives in group behaviour are acted against by unconscious, restrictive solutions. On their account the therapist—by focusing on such key conflicts—helps give members access to the unconscious anxieties and once these have been relieved they can construct more enabling solutions to the shared dilemmas of the group. The idea of focal conflicts, conceived of in these broader terms, has become an integral part of the Group-Analytic model.
(d) The Group-Analytic model
This approach integrates important aspects of the two preceding models but introduces a number of new elements. As Fig. 6.3.6.5 suggests, the therapist is encouraged to address the individual as well as the whole group and considers the more conscious and individual dynamics as well as the unconscious and potentially destructive whole-group dynamics. The approach is guided by an integrated set of concepts relating structure, process, and content to one another in which the group conductor works both as therapist and as group member to foster and cultivate the ordinary language of shared conversational experience. He will at times take up the position of the group’s manager, and at other times he will speak personally as one of its members. Groups may begin with a relatively high level of leadership activity, referred to as dynamic administration, which is flexibly reduced with a decrescendo of responsibility as the group becomes the therapist and the leadership function is devolved upon its membership who becomes active co-therapists in each other’s treatment(44). Figure 6.3.6.6 indicates how, in this approach, at one key moment in the group its theme can focus on structural dynamics that link one member to both the therapist and to the group as a whole. The web of interconnecting dynamics between any one member and all the others, is summarized by ‘the group as a whole’, and this is called on to represent the inter-connecting latticework of relationships that includes all the members and the therapist.
Only gold members can continue reading. Log In or Register to continue