Chapter 153 Iatrogenic Spine Destabilization
The instability that exists after a spine operation may arise from pathologic (intrinsic) or iatrogenic (surgical) processes. Iatrogenic destabilization can result from a variety of sources, such as the destruction of ligaments, muscles, or bone, and the denervation of muscles (Table 153-1).1
TABLE 153-1 Spine Destabilization: Etiology and Management
| Surgery | Reason for Instability | Recommended Management |
|---|---|---|
| Extensive cervical laminectomy | Tension band destruction Facet joint destruction | Laminoplasty or lateral mass plating plus fusion |
| Extensive lumbar laminectomy | Tension band destruction Facet joint destruction | Controversial Possibly dorsolateral fusion Possibly dorsal instrumentation |
| Cervical corpectomy | Bony destruction ALL/PLL destruction | Ventral fusion Ventral instrumentation External orthosis |
| Thoracolumbar total corpectomy | Bony destruction ALL/PLL destruction | Ventral reconstruction plus ventral instrumentation or dorsal instrumentation |
| Corpectomy plus dorsal decompression or total spondylectomy | Extensive bony destruction plus ALL/PLL destruction Facet joint destruction | Circumferential fusion and instrumentation Equal ventral and dorsal instrumentation |
ALL, anterior longitudinal ligament; PLL, posterior longitudinal ligament.
Biomechanical Considerations
One method that is commonly used for evaluating stability is the three-column method of Denis.2 The anterior column is the ventral half of the vertebral body and the anterior longitudinal ligament (ALL). The dorsal half of the vertebral body and the posterior longitudinal ligament (PLL) constitute the middle column. The dorsal column consists of the facet joints and all ligaments dorsal to the spinal canal.
Using the method of Denis,2 significant instability is considered highly likely if two or more columns have suffered substantial injury. The posterior column has true anatomic boundaries, whereas the anterior and middle columns arbitrarily consider halves of a single vertebral body. Many systems for evaluating stability have been devised, but the method of Denis is an example of such a system that is easy to use and widely accepted for clinical application.
Ligamentous Disruption
Ventral Surgery
The ALL and the PLL, as well as the anulus fibrosus, contribute significantly to the stability of the spine.3–5 The PLL is weaker than the ALL and is often intentionally destroyed during dorsal, ventral, or lateral spine surgery. However, the ALL is often not totally disrupted, even with a wide ventral exposure. A strong and wide ligament, the ALL provides a significant proportion of spinal stability in extension. This function may be considered as a tension band that limits extension. As a result, ventral decompressive spine surgery (e.g., corpectomy), which adequately decompresses the dural sac, generally causes a disruption of the PLL, with preservation of at least a portion of the ALL. The width of the PLL significantly narrows in the middle portions of the vertebral body, thus making it susceptible to surgical disruption. In conjunction with existing bony disruption, surgical decompression usually causes significant instability of the spine. The extent of this destabilization can be assessed via intraoperative manipulation, such as vertebral body distraction. If significant instability is iatrogenically created, an interbody strut graft is necessary, with or without supplementation by instrumentation. The PLL limits flexion and distraction.
Dorsal Surgery
Resection of the interspinous ligaments may lead to instability. Although the interspinous ligaments are relatively weak, their long moment arm (i.e., distance from the instantaneous axis of rotation to the ligament attachment site) provides a mechanical advantage with regard to their function as a tension band.1 The capsular ligaments are strong. Although they function through a short moment arm, their relative strength allows them to provide a significant stabilizing effect, if they are intact.
Bone Destruction
Ventral Surgery
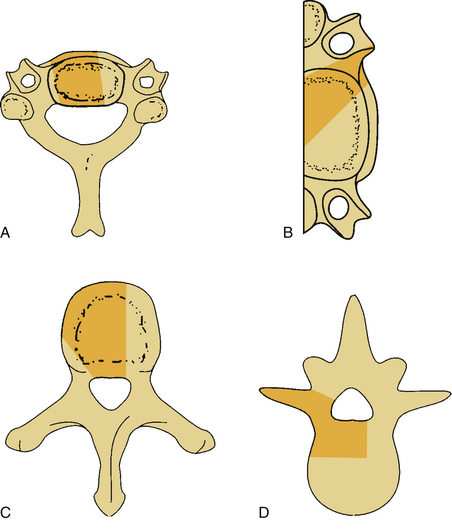
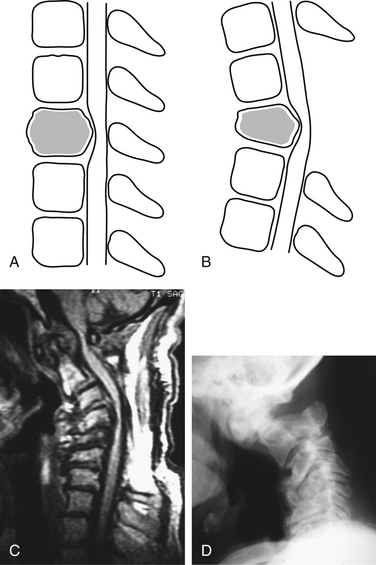
Bone destruction and additional surgical bone removal have a significant impact on spinal stability. Both the amount of vertebral body destruction and its location play an important role in the surgical destabilization process (Fig. 153-1). The first issue is the extent of ventral bony destruction. A complete vertebrectomy causes an obvious instability (see Table 153-1). The extent of instability is closely related to the amount of bone removed.
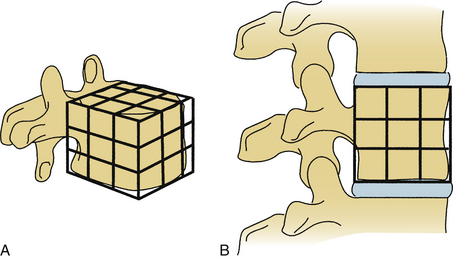
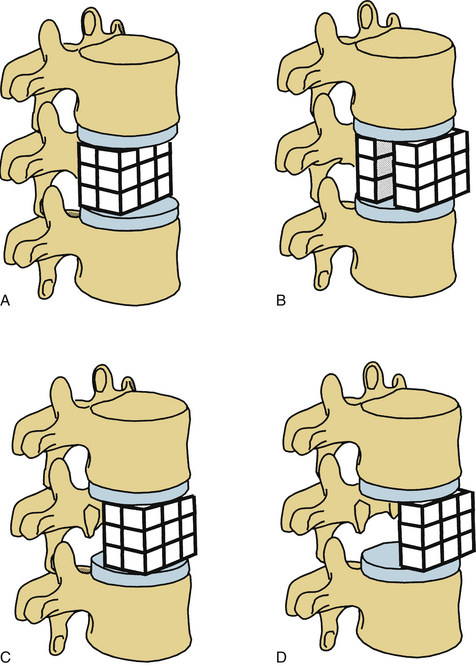
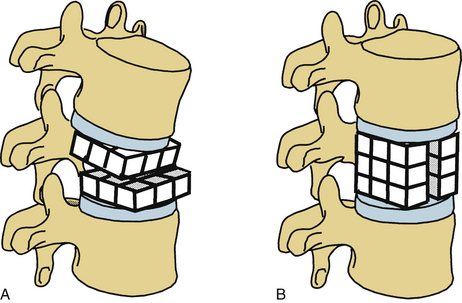
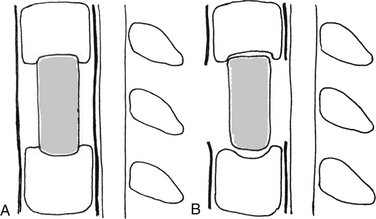
White and Panjabi5 used a three-column model to explain the effects of element disruption on spinal column stability. To determine the effect of a partial vertebral body resection on spinal stability, Benzel1 used a hypothetical design that divides the vertebral body into 27 equal, small cubes (Fig. 153-2). In this regard, resection of the ventral portion of the vertebral body affects spinal stability more than a corresponding resection of the middle or dorsal portion of the vertebral body (Fig. 153-3), because the largest force to which the spine is subjected is that of flexion. The more ventral portion of the vertebral body is farther from the instantaneous axis of rotation, and it therefore exerts its resistance through a longer moment arm in resisting flexion. Also, resection of the middle horizontal section of the vertebral body affects stability more than does resection in the middle vertical sections (Fig. 153-4).
Minimizing bone removal helps decrease postoperative instability. To attain this goal, vertebral body resection in cervical corpectomy should be carefully determined. In this regard, oblique corpectomy is an approach that does not significantly interfere with the stability of the spine.6,7 This approach protects the ventral portion of the vertebral body but sacrifices the dorsal and lateral aspects (see Fig. 153-1B).
As an aside, the uncovertebral joints add stability during extension, lateral bending, and torsion.8 In general, if the (1) ALL, (2) ventral section of the vertebral body, (3) dorsal column integrity, and (4) dorsal column ligaments remain intact, a significant instability does not develop.
Dorsal Surgery
A laminectomy can cause instability because of destabilization of the spine. The frequency of iatrogenic instability is proportional to the width of the laminectomy.9,10 Often, the extent of the injury is not readily apparent shortly after surgery. The prediction of its subsequent occurrence is even less obvious. If a ventral (vertebral body) lesion already exists, the incidence of postlaminectomy kyphosis is even higher.
Laminectomy often creates distortion of the dura mater and spinal cord, with flexion and distraction over the ventral fulcrum (Fig. 153-5). Even in the absence of the ventral pathology, the disruption of the laminae, facet joints, and dorsal ligamentous complex may result in progressive deformity, the so-called postlaminectomy kyphosis (Fig. 153-6). Postlaminectomy kyphosis occurs more commonly in the more mobile portion of the spine—the cervical spine. Laminoplasty may preserve a portion of the dorsal tension band and thereby diminish the instability observed after laminectomy.11 Another alternative that minimizes the destabilizing effect of laminectomy is the addition of a stabilization strategy such as dorsal fusion or external orthosis.
The contribution of the facet joints to dorsal column stability is very important. With axial loading, the anterior and middle columns transmit only 36% of the applied load, whereas each pillar (facet) transmits 32% of the total applied load.12 Therefore, regardless of the region of the spine involved, excessive facet joint resection can result in instability. In the cervical spine, the tolerable limit of resection is one third to one half of the facet joint.10 In the lumbar spine, facet resection may often result in glacial instability. However, the value of fusion and instrumentation after partial facetectomies for spinal stenosis is controversial.13
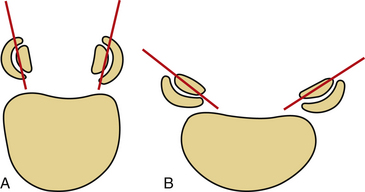
The shape and angulation of the facet joints are also important. A ventral translational deformity is more likely to result if vertically oriented joints and a hyperlordotic posture are present. The L4 and L5 facet joints are sagittally oriented, whereas L5-S1 joints are coronally oriented (Fig. 153-7). Therefore, L5-S1 joints resist translational deformity, whereas L4-5 joints can easily glide on a sagittal plane. Degenerative listhesis frequently involves this level.
Clinical Considerations
Tumor Surgery
An important issue that the spine surgeon cannot avoid is the iatrogenic instability created by radical tumor surgery. Until recently, the surgical treatment of spinal tumors was accomplished predominantly via laminectomy, despite the fact that the neural compression was often ventral to the spinal cord. However, laminectomy was often ineffective. Ventral surgery is often the procedure of choice for treating most bone tumors of the spine.14–16 Because the pathology in most patients with these bone tumors lies ventral to the spinal canal, attempts at tumor resection can cause loss of ventral spinal integrity.
Tumors involving both ventral and dorsal elements cause even greater instability. For oncologic tumor surgery, extramarginal resection of bone tumors of the spine is desirable. Although the spinal cord and nerve roots do not allow such a resection in many instances, there is an increasing trend toward accomplishing total spondylectomies by only a dorsal approach,14,15,17,18 or by circumferential surgery.19,20 Because the iatrogenic destabilization of the spine is so significant in these cases, radical measures to reconstruct and stabilize the spine are mandatory.
Related posts:
 Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


