Influence of Frontal and Sagittal Position of Total Disc Arthroplasty on Clinical Outcomes at 3 Years Follow-Up
S. Aunoble
J.-C. Le Huec
The development of total lumbar disc prostheses has been a logical step in the management of chronic back pain. Clinical results of studies on disc prostheses report patient satisfaction rates, Oswestry scores, and visual analogue assessments for back pain (1,2,3,4,5,6). This motion technology requires an optimal positioning of the implant as reported by Mayer (7). The correlation between the clinical functional result and the position of the implants has rarely been reported. However, such knowledge is essential for understanding the long-term outcome of devices in functional terms (7). This prospective study therefore reports the outcome of 64 Maverick (Medtronic USA) devices implanted between January 2002 and November 2003. Minimum follow-up was 2 years postoperative, with a mean of 24 months (range: 18–36 months).
Material and Method
Sixty-four patients were included in this prospective study and operated in one center by one surgeon. All patients had been suffering from chronic back pain resistant to conservative treatment for at least l year and had received medical and rheumatologic follow-up and rehabilitation physiotherapy.
Contraindications for disc arthroplasty were the following: previous spinal surgery other than discectomy at the painful level, lumbar fracture, permanent symptomatic disc hernia, narrow lumbar canal or isthmic spondylolisthesis, scoliosis greater than 15-degrees Cobb angle, spinal tumor, general or local infection, evolving autoimmune disease, pregnancy, morbid obesity, psychiatric disturbances, and major bone disease.
Inclusion criteria were as follows: age between 20 and 60 years irrespective of gender, symptomatic degenerative lumbar discopathy as evidenced by radiography and magnetic resonance imaging (MRI), failure of conservative treatment given for longer than 12 months, Oswestry score >30%, predominant chronic back pain, and absence of permanent nerve root compression.
There were 64 patients, mean age 44 years (SD 7.1), measuring a mean height of 1.68 m (SD 0.09) and weighing 68 kg (SD 12). There were 39 women and 25 men, all of the Caucasian race. Thirty percent were smokers and 9% had back pain associated
with a work accident. Professionally, 20 were attending work, 21 were absent on account of their back pain, and 23 were no longer able to work. Eighteen patients had had previous spinal treatment: 3 isolated rhizolysis of the posterior facets and 4 disc annuloplasties by radiofrequency at the painful level, one of which was followed by discectomy. There were also 8 patients who had received disc nucleolysis with chymopapain, one of which was followed by discectomy. Twenty-four had a history of abdominal surgery as follows: 13 appendectomies, 2 extrauterine pregnancies, 6 cesarean sections, 3 surgeries for groin hernia, 2 cholecystectomies, 4 tubal ligations under coelioscopy, and 2 hysterectomies.
with a work accident. Professionally, 20 were attending work, 21 were absent on account of their back pain, and 23 were no longer able to work. Eighteen patients had had previous spinal treatment: 3 isolated rhizolysis of the posterior facets and 4 disc annuloplasties by radiofrequency at the painful level, one of which was followed by discectomy. There were also 8 patients who had received disc nucleolysis with chymopapain, one of which was followed by discectomy. Twenty-four had a history of abdominal surgery as follows: 13 appendectomies, 2 extrauterine pregnancies, 6 cesarean sections, 3 surgeries for groin hernia, 2 cholecystectomies, 4 tubal ligations under coelioscopy, and 2 hysterectomies.
Levels to be operated were the following: disc prosthesis L5-S1 (35 cases), L4-5 (14 cases), and arthrodesis L5-S1 with disc prosthesis at L4-L5 (13 cases), and prosthesis at L3-4 (2 cases). All had received radiologic, static, dynamic and load-bearing evaluation, in addition to MRI. Preoperative MRI was used to assess the state of the disc.
Radiography was used to examine mobility during flexion-extension at the level of the device and the two adjacent levels. Measurements performed by an independent radiologist on anteroposterior (AP) and lateral radiographs were accurate to 3 degrees for angles and 3 mm for distances. Implant position was defined according to coronal x-rays as shown in Fig. 19.1. In this way, the keel of the device serves as a landmark to establish its position. The symmetrical center of the vertebra corresponds coronally to the midpoint of its width. The distance between the midpoint of the vertebra and the keel of the device is related to the radius of the vertebra and expressed as a percentage. When the device is centered, its degree of lateralization is 0%. The more lateralized it is, the closer it is to a score of 100%. Our arbitrary rating system is as follows: 0 to 9%, well centered; 10 to 19%, moderately off center; and 20% and above, off center. Implant position was defined on lateral x-rays as shown in Fig. 19.2. The position of the device was defined according to the distance between its posterior edge and the posterior edge of the inferior vertebral body of the segment. To obtain a value independent from the radiographic enlargement factor, measurements were related to the size of the keel of the device, which was constant whatever the model. If the device was too posterior (in the vertebral canal), the distance was expressed as a negative value. A distance from
the posterior edge of the vertebra between 4 and 7 mm was considered to represent a moderately correct position, whereas a distance <4 mm was taken to be satisfactory. Any distance >7 mm was considered inadequate.
the posterior edge of the vertebra between 4 and 7 mm was considered to represent a moderately correct position, whereas a distance <4 mm was taken to be satisfactory. Any distance >7 mm was considered inadequate.
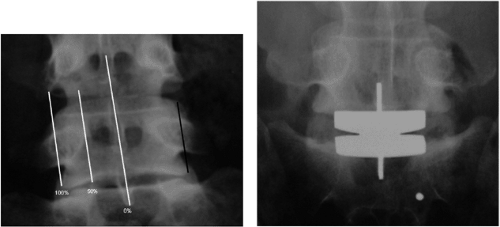 FIGURE 19.1 |
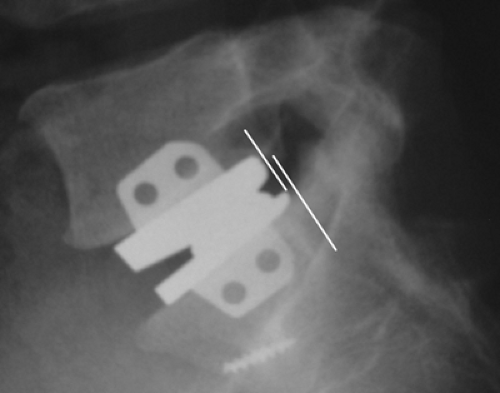 FIGURE 19.2 |
The prosthesis is inserted by a mini-invasive anterior approach (11) with complete discectomy and release of the discal space. The patient is positioned supine in the so-called French position, with legs bent and open laterally (12,13). The incision is longitudinal or horizontal crossing the midline, 7 to 8 cm long. After vertical incision of the rectus abdominis sheath, the muscle is retracted laterally to reach the common fascia of the external oblique muscle. The peritoneal sac is pushed to the contralateral side with the ureter and the hypogastric plexus. To reach L5-S1, the left iliac vein must be carefully retracted and the medial sacral vessels ligated. At the L4-5 level, the surgeon must pay attention to the ascending lumbar vein, which is located at the corner of the psoas belly and the left iliac vein. This important collateral must be ligated. The segmental vessels at L4 and L5 must also be ligated to allow retraction of the aorta and vena cava. The anterior part of the disc is opened according to the size of the templates, then the anterior annulus and nucleus are removed using disc rongeur, Kerrison, curettes, and a scraper. It is not necessary to open the posterior longitudinal ligament, but it must be detached from the posterior border of the endplates using the specific instruments. The mobility of the disc space is tested with a spreader under C arm control. The midline is checked with AP fluoroscopy. A dedicated instrument is introduced in the disc space and makes it possible to create a parallel distraction of the disc, thus restoring the disc height. The upper or the lower keel cutter is slid onto a guide and impacted into the vertebral body to prepare the bed for the fin of the prosthesis. The position of the implant on the lateral view is controlled on the fluoroscopic image and the correct position is a distance in between the posterior part of the inferior vertebral endplate and the posterior part of the implant inferior to 4 mm. The prosthesis is impacted into the prepared disc space under fluoroscopic control. The retractors are carefully removed and the rectus abdominis fascia and subcutaneous fat are closed with drainage.
The implant used is a metal on metal disc prosthesis Maverick (Medtronic, Memphis, TN) made of cobalt chrome, with a ball and socket design. The prosthesis has a fixed posterior center of rotation located below the lower endplate. The production of wear debris is very low without epidural reaction on animal studies (3,12,14).
All patients were seen at 1, 3, and 6 months, then 1 and 2 years, with assessment of pain, according to a visual analogue scale (VAS), neurologic function, Oswestry scores, and the SF36 (15). Clinical success was taken to be a 25% improvement on the Oswestry score, and 2 points improvement on the VAS back pain score, that is, the success rate defined by the U.S. Food and Drug Administration (FDA) in a randomized prospective study concerning the SB Charité prosthesis (16). Degree of patient satisfaction was noted, as were need of antalgics and duration of treatment with antalgics or anti-inflammatory agents. All patients received postoperative physiotherapy from 1 week postoperative and wore a supple girdle for 6 weeks. Statistical analysis was with the t test and the chi-square test.
Results
All the patients underwent follow-up examinations preoperatively, immediate postoperatively, and at 2-years’ follow-up. Oswestry score preoperatively and at 2-years’ follow-up was 43.8 and 23.1, respectively (p < 0.05). Low back pain improved from a mean VAS of 7.6 ± 1.7 preoperatively to 3.2 ± 1.8 at 2 years (p < 0.05). Mean visual analogue leg pain score decreased from 3.9 to 2.1 at 2 years (p < 0.05). Mean daily duration of back pain decreased from 70% to 40% (p < 0.05). Daily duration of leg pain decreased from 36% to 20% (p < 0.05). According to the FDA criteria (>25% improvement of Oswestry score and >2 points of back pain on VAS) (17), the success rate was 75% (p < 0.05). Improvement in back pain directly affected the improvement in Oswestry score (p = 0.008) (Table 19.1).
Evolution of SF score was weighted according to gender and age of the patient. An improvement >15% was taken as success.(7,16) Thus, 85% of patients experienced physical improvement at 1 year, and improvement of mental health was noted in 43%. The mean hospital stay was 4.6 days (3 to 10 days).
Complications
Minor intraoperative complications were noted due to the surgical approach in 11 cases. There was never any breakage of the device. No implant had to be removed or surgically revised.
Consumption of antalgics was reduced overall because no patient needed any morphine-based drugs postoperatively, whereas 62% were taking them preoperatively. With regard to resumption of professional activity, 63% returned to work, mean time to return to work being 5 months (range: 2 months to 1 year). When the Oswestry score was improved by ≥ 25%, there was a 44.4% chance of returning to work. When the score was improved 75%, the chance was 73% (p = 0.004). Factors influencing the clinical result in terms of success were as follows: young age associated with a good result (p = 0.05) and female gender associated with better results (p = 0.003). On the other hand, previous spine surgery decreased the chance of having a good result (p = 0.005), whereas being off work before the intervention did not influence clinical outcome (p = 0.14).
Related posts:
 Adjacent Level Disc Biomechanics
Adjacent Level Disc Biomechanics
 Nucleus Pulposus Regeneration: Present Limitations and Future Opportunities
Nucleus Pulposus Regeneration: Present Limitations and Future Opportunities
 Prosthetic Disc Nucleus: Treatment with the Anterior Approach
Prosthetic Disc Nucleus: Treatment with the Anterior Approach
 Total Lumbar Disc Arthroplasty: Overview of Clinical Results for Existing Implants
Total Lumbar Disc Arthroplasty: Overview of Clinical Results for Existing Implants
 A New Approach to Lumbar Disc Prosthesis
A New Approach to Lumbar Disc Prosthesis
 Posterior Nonfusion Stabilization of the Degenerated Lumbar Spine with Cosmic
Posterior Nonfusion Stabilization of the Degenerated Lumbar Spine with Cosmic
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


