INSOMNIA: A COMPLEX PROBLEM AND A CHALLENGE TO TREAT
Many times insomnia is difficult to resolve, and all physicians have many patients with insomnia. This chapter aims to help the professional who is confronted with an insomniac to move from a chief complaint of insomnia to a plan for the patient’s treatment, or to a referral for treatment. We mention the option of a referral for treatment because of our assumption that not all physicians will choose to treat people with persistent or severe insomnia.
Sleep is sensitive to disturbance by many internal influences, such as excessive worry, excessive anxiety, and a depressed mood. Sleep can also be disturbed by many external influences, for example, transient stress, an important life event, excessive noise, high or low room temperature, an uncomfortable bed, high altitude, jet lag, drug withdrawal, and sleeping in unfamiliar surroundings. Several types of etiologic factors can cause chronic difficulty sleeping, including circadian rhythm disorders, psychiatric disorders, pharmacologic agents, physical illnesses, sleep-related physiologic disorders, and negative conditioning effects; there are subtypes under each of these types of etiologic factors.
Subtypes of insomnia have specific therapies; it is not accurate to view insomnia as one general problem of difficulty sleeping that has only one treatment. The term insomnia has several meanings. First, it is common and appropriate to consider insomnia as a stereotype for disturbed sleep. Second, insomnia is a clinical symptom for over 30 sleep disturbance diagnostic subtypes. Finally, people with insomnia represent a large set of sleep disorders; hence, it is proper to speak of the insomnias, which are disorders that present with an insomnia complaint. The insomnias have varied causes and specific treatments with proved effectiveness for different diagnostic subtypes.
Although insomnia can be difficult to resolve, not all cases warrant referral to a specialist. As with other widespread health problems, most people with insomnia are initially seen by primary care physicians, who, of course, are not sleep specialists. A clinical assessment of limited intensity is suitable for the initial insomnia evaluation and adequate for the initial treatment selection. The cases of recent onset, and the less severe cases, can be successfully evaluated and successfully treated by physicians in general practice. The more chronic and the more severe cases may need to see an insomnia specialist.
CLINICAL EPIDEMIOLOGY AND SIGNIFICANCE
The high prevalence of insomnia is well documented; population surveys estimate that one-third of all adults have one or more episodes each year (1). In one of the best US surveys, 15% reported having a serious problem with insomnia during the past year (2). Insomnia increases with age. In middle-age samples, the frequency of chronic insomnia is estimated to be around 10% (3). Clinically, significant insomnia prevalence in older adults is estimated at 25% and higher (1,2). Insomnia is common enough in late life to be one of the negative changes that characterize the experience of aging. In a recent US poll, 67% of the adults over age 55 reported having symptoms of sleep disorders at least a few nights a week, but only 8% had been diagnosed with a sleep disorder, and fewer received treatment (4).
Clinical insomnia not only causes nights of restless, broken sleep and frustration; daytime sequelae include depressed mood, anxiety, daytime fatigue, irritability, reduced concentration, and memory complaints (5,6). Daytime functioning impairment that patients attribute to insomnia can affect the physical, emotional, cognitive, occupational, and social areas of life (7,8).
PRIMARY AND COMORBID INSOMNIA
Insomnia disorders are typically categorized according to their etiology. Primary insomnia refers to two types of cases: (a) a situation where basic features of a primary insomnia have been identified, or (b) a situation where underlying causes for secondary insomnia have been ruled out, thus revealing that the insomnia is an independent disorder. Primary insomnia is sometimes referred to as pure insomnia, to indicate that difficulty sleeping is at the core of the disorder. These cases are some of the most difficult insomnias to treat. When physicians refer cases to insomnia specialists, they are often those judged to be chronic primary insomnia.
The majority of people with a chronic complaint of insomnia are found to have secondary or comorbid insomnia (9). However, it is difficult to discriminate primary insomnia co-occurring with another disorder (comorbid insomnia) from insomnia caused by another disorder (secondary insomnia). A recent review analyzes the challenges of this diagnostic task (10).
Until recently, when another medical or psychiatric condition was present in a patient with insomnia complaints, the insomnia was assumed to be secondary. The standard course of treatment for secondary insomnia focused on the underlying factor or condition believed to have caused the patient’s poor sleep. As a consequence, direct treatment of the insomnia was delayed because of the expectation that the patient’s sleep would improve once the other “primary” condition was treated. However, secondary insomnia does not consistently resolve after treatment for the presumed primary condition (11). In addition, recent research demonstrates the effectiveness of direct treatment for secondary and comorbid insomnia (11,12). In light of these issues, the 2005 National Institutes of Health (NIH) State-of-the-Science conference on chronic insomnia recommended that the term “secondary insomnia” be replaced with the more appropriate term “comorbid insomnia” (13). Current treatment guidelines have followed suit by recommending direct treatment for both primary and comorbid insomnia, regardless of etiology (14,15).
To avoid delayed treatment for persistent insomnia, we recommend that when secondary or comorbid insomnia is suspected, treatment should be pursued for the condition perceived to be contributing to the insomnia; direct treatment should also be pursued for insomnia. The direct treatment for insomnia will prevent chronic, untreated insomnia.
TRANSIENT AND SHORT-TERM INSOMNIA (PROS AND CONS ON TREATMENT)
Most insomnia episodes last for ≤1 month (2). These are highly prevalent and are classified as transient or short-term insomnias. When an episode lasts for >4 weeks, it is termed chronic or persistent insomnia.
The more brief insomnias raise the questions of treatment need and timing—whether to treat an insomnia complaint, and whether to treat it right away when the patient first presents versus a decision not to treat, or at least to delay a treatment choice until the problem is shown to be more persistent. There are two common responses to these questions.
First, when the decision is “no” to treatment for short-term insomnia, limited assistance will typically be offered. General sleep management advice and a supportive manner are routinely offered. General sleep management advice typically includes sleep hygiene advice, and may include some basic behavioral treatment advice (e.g., stimulus control instructions and sleep restriction guidelines). When treatment is not offered, there are implied assumptions: (a) that treatment is not necessary for symptom relief and (b) that treatment is not necessary to prevent the problem from persisting or worsening.
When the decision is “yes,” and treatment is offered for an insomnia of recent onset, the service provider typically seeks two types of benefit: sure and possible benefits. Certainly, this early treatment can be counted on to provide symptom relief and alleviate emotional distress. A common treatment package includes a trial with sedative—hypnotic medication (16) and basic sleep hygiene advice. The second, and more speculative type of benefit is preventive. Some physicians begin treatment early in the history of insomnia as part of the effort to prevent chronic insomnia.
A decision to provide no treatment often offers the patient only support and sleep hygiene advice. A decision not to treat short-term insomnia is reasonable, based on statistics that, without treatment, most transient and short-term insomnias do not progress to chronic insomnia (17).
The decision to treat an insomnia of recent onset is a clinical one, based on patient distress and professional judgment about need for intervention. Prevention of chronic insomnia is an additional treatment goal in some cases (16). There is no research to document long-term benefits from early treatment, nor are there data showing long-term negative consequences from early treatment.
MODEL OF CAUSES AND TREATMENTS FOR INSOMNIA
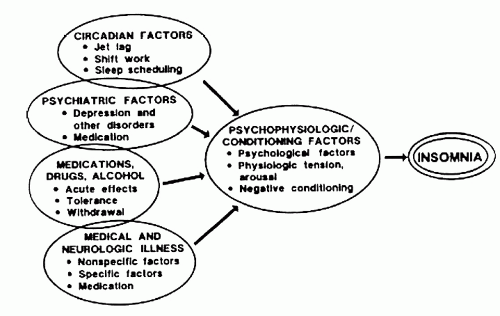
Buysse and Reynolds (18) present a conceptual framework within which to examine insomnia cases. A graphic portrayal of their ideas is presented in Figures 13-1 and 13-2. Figure 13-1 summarizes the varied types of etiologic factors; Figure 13-2 is discussed later (see Principles for Treatment Planning). Figure 13-2 presents a multifactor model of insomnia treatment. These figures and the overview of insomnia etiologies that they portray can help a professional organize in preparation for the tasks of insomnia evaluation and treatment.
FIGURE 13-1 Several etiological factors may contribute to the development of insomnia. Psychophysiologic and behavioral factors often perpetuate insomnia that had its origins in a medical, psychiatric, or circadian disturbance. (Reprinted from Buysse DJ and Reynolds CF. Insomnia. In: Thorpy MJ, ed. Handbook of sleep disorders. New York: Marcel Dekker, 1990:375-433, with permission.)
Figure 13-1 shows causes of insomnia. It begins with four general types of etiologic factors commonly noted in people with insomnia (circadian, psychiatric, pharmacologic, and medical/neurologic illness). These four factors are portrayed as common precipitating factors for episodes of insomnia. In addition, the stereotypic insomnia experience includes psychophysiologic and conditioning factors that may precipitate and that often perpetuate an insomnia.
Psychophysiologic and conditioning factors characterize single-diagnosis primary insomnia, and they characterize the conditioned insomnia that is commonly overlaid on other types of persistent insomnia. Such overlay often causes multiple-diagnosis chronic insomnia (Fig. 13-1).
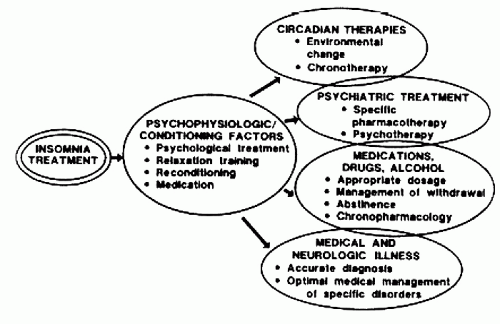
FIGURE 13-2 Treatment of insomnia must often address multiple etiological factors. Treatment aimed at psychophysiologic behavioral factors is often appropriate, even when medical, psychiatric, or circadian disturbance is present, since these behavioral factors may perpetuate other types of insomnia. (Reprinted from Buysse DJ and Reynolds CF. Insomnia. In: Thorpy MJ, ed. Handbook of sleep disorders. New York: Marcel Dekker, 1990:375-433, with permission.)
The psychophysiologic and conditioning factors include: (a) psychologic characteristics (such as subclinical anxiety and low mood), (b) physiologic tension/arousal, and (c) a history of negative conditioning (caused by frequent nights with excessive amounts of time spent lying awake). Negative conditioning is sometimes compounded by learning negative sleep habits (poor sleep hygiene), such as staying in bed late in the morning, naps, irregular bedtimes, and trying too hard to sleep. The physiologic tension/arousal of insomnia varies across individuals and may include cognitive overarousal (e.g., “mind racing,” “thinking about all kinds of things,” and “thoughts jumping from topic to topic”), physiologic overarousal (e.g., tense muscles, restlessness, and “feel wide awake”), and arousability/sensitivity to stimuli (such as environmental sounds, temperature, light, and bedcovers).
Buysse and Reynolds emphasize that the most important components of chronic insomnia may be the psychophysiologic and behavioral/conditioning factors, since they “often perpetuate an insomnia, which had its origin in a medical, psychiatric, or circadian disturbance” (18, p. 380). The behavioral therapies for insomnia (see Behavioral Treatments for Persistent Insomnia) are designed to reverse the behavioral/conditioning and psychophysiologic factors that can be the key perpetuating factors for a chronic insomnia.
Figure 13-2 (see Principles for Treatment Planning) outlines the types of insomnia treatment that address the varied insomnia causes shown in Figure 13-1. Successful insomnia treatment often contains only one technique such as pharmacotherapy, stimulus-control behavior therapy, or medical treatment for a sleep-related physiologic disorder (e.g., periodic limb movement disorder [PLMD] and restless legs syndrome [RLS]). One treatment technique is the simplest treatment plan. The complexity of factors contributing to chronically disturbed sleep often necessitates a multicomponent treatment plan. Multiple diagnoses for a person with chronic insomnia are frequently noted, which is another reason why “treatment for insomnia must often address multiple etiological factors” (18, p. 408).
CATEGORIES OF INSOMNIA SUBTYPE
The International Classification of Sleep Disorders, Second Edition (ICSD-2) presents 11 categories of insomnia disorders, two of which are unspecified (Table 13-1). The nine major subtypes of insomnia listed in the ICSD-2 are described in the following sections and prevalence and typical course discussed. The subtype descriptions are based on the ICSD-2 (17). Although the ICSD-2 does not include a separate category for insomnia related to other primary sleep disorders, the following sections include a discussion of insomnia associated with circadian rhythm disorders and sleep-related physiologic disorders.
As an aid to diagnosis and treatment planning, insomnia subtypes are grouped and discussed according to presumed etiology. The etiologic factors for the following sections include (a) transient or short-term factors, (b) psychophysiologic and/or conditioning factors, (c) associated mental disorder, (d) drug or substance, (e) medical disorder, (f) circadian rhythm disorder, and (g) sleep-related physiologic disorder. These groupings will also help lay the groundwork for our discussion of assessment and treatment selection.
TABLE 13-1 INSOMNIA DISORDERS IN THE ICSD-2
Adjustment insomnia (acute insomnia)
Psychophysiological insomnia
Paradoxical insomnia
Idiopathic insomnia
Inadequate sleep hygiene
Behavioral insomnia of childhood
Insomnia due to mental disorder
Insomnia due to drug or substance
Insomnia due to medical condition
Insomnia not due to substance or known physiological condition, unspecified (nonorganic insomnia, NOS)
Physiological (organic) insomnia, unspecified
Transient or Short-term Factors (The Most Frequent Cause)
Adjustment Insomnia
Adjustment insomnia, also called acute or transient insomnia, is the most common type of insomnia. The sleep disturbance has a relatively short duration (<3 months) and is correlated with a clearly identifiable stressor. Precipitating stressors can include psychological, social, medical/physical, or environmental changes, such as a child preparing to begin a new school year or someone moving to a new location, facing an important evaluation, or dealing with interpersonal problems or bereavement. To diagnose an adjustment sleep disorder, the insomnia must be a clear change from the patient’s norm. However, once the precipitating stressor is resolved or the individual learns to adapt to an ongoing stressor, the patient’s sleep is expected to return to normal. All people are subject to having adjustment insomnia. Epidemiologic studies suggest that one-third of adults have at least one episode of transient insomnia each year (2).
Serious complications are usually absent. If left untreated, possible complications include negative conditioning of associations with the bedroom and decreased confidence in the ability to sleep normally, consequences which could favor the development of persistent insomnia. However, serious medical or psychologic complications are believed to be rare, unless an adjustment sleep disorder is overlaid on preexisting medical or psychiatric illness (17).
Insomnia Related to Psychophysiologic and/or Conditioning Factors
The first four subtypes of insomnia in this section are often referred to collectively as primary insomnia. They represent the insomnias that have been formally designated as exemplars of persistent primary insomnia, or pure insomnia (17); the first, psychophysiological insomnia, is considered the most stereotypic primary insomnia.
Psychophysiological Insomnia (The Classic Form of Pure Insomnia)
Psychophysiological insomnia (19) is the most common type of persistent primary insomnia and considered the prototype for primary insomnia. Psychophysiological insomnia is defined as a persistent, or chronic, disorder of somatized tension, maintained by learned sleep-preventing associations. Based upon repeated negative experiences with difficulty sleeping, the learned associations can be established either to internal mental contents (e.g., based upon repeated associations between thoughts of bedtime and aroused anticipation of difficulty sleeping) or to external stimuli (such as many experiences associating the bedroom environment with excess arousal during the night).
Conditioned associations to external stimuli are often caused by the frequent association of sleeplessness with situations and behaviors related to sleep, which can establish conditioned excess arousal in the prebedtime period. After many repetitions, lying awake in one’s bedroom may cause conditioned excess arousal, as may behaviors that lead up to bedtime, such as brushing teeth, preparing the bedroom, or turning off the lights. Occasionally, a person with insomnia will temporarily escape this conditioned arousal and sleep well when sleeping in unfamiliar surroundings that have not been previously associated with insomnia (e.g., when visiting the home of a friend or relative).
Learned associations to internal mental contents are mainly conditioned overconcern about the inability to sleep. This overconcern can cause a circular pattern wherein difficulty sleeping leads to more effort to obtain sleep, which causes an increase in arousal, and less ability to sleep. This pattern is often referred to as trying too hard to sleep, and it is associated with a complementary ability to fall asleep more easily when not trying. For example, a person who frequently stays awake at night when trying to sleep may become drowsy when listening to a lecture or watching television, despite an intent to stay awake. The drowsiness may represent an escape from the anxiety and arousal often associated with trying to sleep.
As a complication of psychophysiological insomnia, excessive use of hypnotics or use of alcohol as a sleep aid is often noted. Tranquilizers may be used in the daytime to decrease somatized tension, and caffeine or stimulants may be used to combat fatigue.
Among patients referred to sleep disorders centers, about 15% of people with insomnia complaints receive a diagnosis of psychophysiological insomnia (20). It is estimated that 1% to 2% of the general population experience psychopysiological insomnia (17). Among all individuals who experience a transient sleep disorder, it is not known how many go on to develop psychophysiological insomnia.
The widespread occurrence of learned sleep-preventing associations represents, over the course of persistent insomnia episodes, a component that is added to the initial pattern of sleep disturbance for most chronic insomnias. Learned sleep-preventing associations, while the key defining feature of psychophysiological insomnia, also play an important role in the other forms of insomnia, based upon the common experience of negative conditioning.
Psychophysiological insomnia and the other primary insomnias are typically diagnosed by exclusion, after all the causes of secondary insomnia have been ruled out. In addition to single-diagnosis psychophysiological insomnia, this type of insomnia is often present in multiple-diagnosis cases of chronic insomnia, due to the overlay of conditioned sleep-preventing associations developed over time.
When trying to determine the most basic factor contributing to a possible psychophysiological insomnia, a common differential concerns psychiatric disorders that include sleep disturbance. When an affective disorder, generalized anxiety disorder, or other mental disorder is present, psychiatric treatment will usually take precedence over treatment for psychophysiological insomnia. A recent study challenges the precedence for psychiatric treatment that causes delay in insomnia treatment. The results of Lichstein et al. (21) suggest that simultaneous treatment for psychiatric disorder and behavioral treatment for insomnia can be successful.
Paradoxical Insomnia
Paradoxical insomnia (22) is a disorder in which a subjective complaint of insomnia occurs, but objective sleep laboratory results do not show significant difficulty falling asleep or staying asleep. In the morning after polysomnography (PSG, the term for physiologic sleep recordings), the patient will report the insomnia problem occurred during the night. The prevalence of this disorder is not known because most insomnia patients are not referred for sleep laboratory testing.
The apparent conflict between the subjective and objective findings has not been explained. The most common explanation is that these patients experience a type of objective problem that is not measured by standard PSG measures; for example, perhaps experiential awareness that persists during sleep, which is not measurable by standard sleep recordings, contributes to a perception of being awake. This hypothetical unmeasured cognitive activity perhaps could resemble the cognitive awareness of one’s own dreaming that occasionally occurs during rapid eye movement (REM) sleep, during what is known as a lucid dream—but the sleep state misperception patient does not have the unusual mental activity that cues a lucid dreamer to the presence of sleep (as well as being a cue for the lucid dreamer to the presence of dreaming). Perhaps paradoxical insomnia patients have other physiologic abnormalities during sleep that are not detected by recording methods currently in use.
Some research has shown similar subjective results from behavioral treatment for psychophysiological insomnia and behavioral treatment for paradoxical insomnia patients (23). The psychological evaluation results with paradoxical insomnia do not reveal evidence of psychopathology. A preliminary study suggested that the use of educational therapy with viewing of the video portion of the sleep study with the patient may be a helpful treatment modality in this difficult to treat disorder (23a). Before treating for paradoxical insomnia, special care should be taken to rule out insomnia related to mental disorder.
TABLE 13-2 DAILY LIVING ACTIVITIES THAT ARE INCONSISTENT WITH THE MAINTENANCE OF GOOD QUALITY SLEEP
1.
Frequent napping
2.
Variable bedtimes or variable morning risetimes
3.
Frequently spending an excessive length of time in bed
4.
Regular use of sleep-disruptive substances near bedtime (e.g., alcohol, tobacco, and caffeine)
5.
Exercise too near bedtime
6.
Stimulating activities too close to bedtime
7.
Use of the bed for non-sleep-related activities (such as watching television, reading, and snacking)
8.
Using an uncomfortable bed
9.
Poor control of the bedroom environment (e.g., too much light, heat, cold, or noise)
10.
Performing activities that demand strong concentration near bedtime
11.
Allowing oneself to persist in sleep-preventing mental activities while in bed, such as thinking, planning, and reminiscing. (When these mental activities persist, it is best to get out of bed for a while and do something relaxing until sleepy.)
Idiopathic Insomnia
Idiopathic insomnia (24) is a rare, lifelong inability to obtain adequate sleep. It typically begins at birth, or by early adolescence at the latest, and persists into adulthood. It is presumably due to an abnormality in the neurologic regulation of sleep (the sleep-wake system). The insomnia cannot be explained by childhood psychological trauma or by medical problems that chronically disturb the sleep-wake system, such as pain or allergies.
Chronically poor sleep leads to a general decrease in sense of well-being; there can be low mood, decreased motivation, decreased vigilance and concentration, low energy, and fatigue. However, as long as sleep disturbance remains mild to moderate, psychologic adjustment remains in the normal range. If idiopathic insomnia is severe, daytime functioning may be severely disrupted and depressive features may be prominent.
The population prevalence of idiopathic insomnia is unknown, but research suggests that approximately 0.7% of adolescents and 1.0% of young adults may have this condition (25). Idiopathic insomnia is rarely observed in a pure form. The lifelong difficulty almost always causes complications that compound the problem, such as conditioned sleep-preventing associations and sleep-disruptive psychiatric symptoms. Hypnotics are often used excessively and, often, there is excessive alcohol intake in an effort to promote sleep.
Inadequate Sleep Hygiene
Inadequate sleep hygiene is a sleep disorder resulting from habits and activities of daily living that are inconsistent with obtaining good quality sleep and that work against maintaining full daytime alertness.
Sleep hygiene habits are important health knowledge; they include positive and negative sleep management behaviors that are under an individual’s control. Negative sleep hygiene behaviors can be classified in two general categories: (a) practices that increase general level of arousal during nocturnal sleep times (e.g., regular daytime naps) and (b) practices that disrupt the sleep pattern within an individual night (such as alcohol) or influence the pattern across nights (such as a frequently changing sleep schedule).
Table 13-2 presents a representative list of negative sleep hygiene practices. This list is based upon material from the ICSD-2 (17).
When sleep hygiene is grossly inadequate, it can easily be revealed during a clinical evaluation. For example, a grossly excessive length of time spent in bed, frequent naps, or high variability in the time of arising will be obvious. Mild deficiencies that cause sleep disturbance may be missed during an initial interview. Daily sleep logs, when filled out for 2 weeks, can greatly help in the thorough assessment of the scheduling aspects of sleep hygiene.
Inadequate sleep hygiene behaviors may precipitate an episode of insomnia, and they may help perpetuate insomnias with varied etiologies. It is important to assess sleep hygiene in all insomnia patients because some negative sleep habits start after a sleep problem begins, in response to an episode of insomnia (such as napping and trying to sleep late in the morning—both habits that can develop due to seeking more sleep). These efforts to cope with the problem can help perpetuate the insomnia.
The prevalence of inadequate sleep hygiene disorder is not known, although it is believed to be a fairly common precipitant of insomnia episodes and a frequent contributing factor in persistent insomnia. In many cases, multiple factors have a cumulative effect that causes clinically significant insomnia, and inadequate sleep hygiene is common among the causal factors.
Behavioral Insomnia of Childhood
There are two types of behavioral insomnia of childhood, both of which have an identified behavioral etiology. The sleep-onset association type results from inappropriate sleep associations (e.g., falling asleep with a bottle and sleeping in the parents’ bed) that lead to difficulties falling asleep when the associated object or routine is not present for the child. The limit-setting type of behavioral insomnia often presents with a child’s stalling or refusal to go to bed and is related to insufficient or inappropriate limit setting by a caregiver.
The onset of behavioral insomnia of childhood can occur any time during late infancy (usually not before 6 months of age) through childhood. Behavioral insomnia of childhood is diagnosed based on parental or adult caregiver reports of the child’s insomnia symptoms. The child’s nighttime difficulties often disrupt the parents’ sleep, and may be accompanied by daytime problems with limit setting or child behavior. Because of the heterogeneity in the course of behavioral insomnia across a child’s development and the unique treatment needs of children and families, this insomnia disorder is not discussed further in this chapter (see ref. (26) for additional information on childhood sleep problems).
Insomnia Due to Mental Disorder
Most psychiatric disorders can have associated sleep disturbance. The ICSD-2 includes six main categories of mental disorders that are commonly seen in patients presenting with sleep complaints and need to be considered in differential diagnosis (17). These categories are mood disorders; anxiety disorders; somatoform disorders, schizophrenia/other psychotic disorders; disorders usually diagnosed in infancy, childhood, or adolescence; and persistent personality disorders. The four categories most commonly associated with insomnia are discussed now.
Mood Disorders Associated with Sleep Disturbance
Major depression and dysthymia, mania, and hypomania, as well as other mood disorders, typically are associated with insomnia (27). In rare cases, excessive daytime sleepmess (EDS) is associated with a mood disorder.
The difficulty sleeping associated with mood disorders includes two general patterns of insomnia that can help indicate the presence of depression and mania. In the depression pattern, there is difficulty falling asleep, sleep maintenance disturbance, and early morning awakening that prematurely ends the night’s sleep (also termed early final awakening or terminal insomnia). The mania pattern shows sleep-onset insomnia and short sleep duration (sometimes with severely reduced total sleep time [TST]).
Frequent awakenings and early morning awakening are the most characteristic sleep features of major depression. Waking up well before the planned time of arising followed by inability to return to sleep is the cardinal sleep complaint for major depression. Most depressed patients complain of nocturnal restlessness and daytime tiredness. In contrast, mania and hypomania patients, despite low TST, do not complain about the lack of sleep and report feeling rested and alert during the daytime. Despite their severe insomnia and daytime tiredness, most depressed patients are not objectively sleepy during daytime sleepiness testing with the Multiple Sleep Latency Test (MSLT) (28).
Among depressives, in general, younger patients are more likely to experience difficulty falling asleep at bedtime, relative to more elderly patients who experience greater difficulty with during-the-night awakenings. The characteristic pattern of insomnia associated with depression is frequently a very early sign of mood disorder, often appearing before clinical depression has become clearly established. With initiation of antidepressant medication, the insomnia complaint tends to improve more rapidly than the mood disturbance. Clinical experience indicates that at least 90% of patients with mood disorders have sleep disturbances at some time.
PSG recordings of depressed patients show abnormalities on several features of REM. The night’s first period of REM sleep begins early (i.e., there is a short REM latency). Early onset of REM is the most characteristic feature of sleep laboratory results for depressed patients. Increased density of rapid eye movements during REM sleep is another abnormality associated with depression. Particularly because of REM abnormalities, PSG can be useful in confirming a mood disorder diagnosis. The PSG data can provide evidence of a biological component to the disorder, in support of somatic therapies for depression.
Anxiety Disorders Associated with Sleep Disturbance
The anxiety disorders (including panic disorder, generalized anxiety disorder, acute stress disorder, and posttraumatic stress disorder) are characterized by chronic anxiety and avoidance behaviors. The associated sleep disturbance is characteristically a sleep-onset or a sleep-maintenance insomnia, resulting from excessive anxiety, hypervigilance, or apprehensive expectation about life events. Typical sleep symptoms include frequent awakenings (some with anxious dreams), ruminative thinking, and anxiety attacks while awake during the night.
Specifically, panic disorder is characterized by discrete episodes of intense fear or physical discomfort, which can occur unexpectedly. Panic episodes can be associated with sudden awakenings from sleep, followed by persistent arousal and difficulty returning to sleep (29).
Some types of sleep-related fear episodes need to be differentiated from awakenings related to panic disorder. Sleep terror episodes begin with a loud scream or yell during deep, nondreaming sleep. Sleep terror patients do not have daytime panic symptoms. Panic attacks are also not REM-related nightmares. Panic attacks tend to occur in non-REM stage 2 or 3 sleep and do not include dreamlike mental content.
For all the anxiety disorders, once the sleep disturbance has become chronic, conditioned arousal to the sleep environment may also be present. This conditioned sleep-preventing response is in addition to the excessive arousal of an anxiety disorder. This negative conditioning is not the most basic sleep-disturbing factor.
Anxiety disorders are chronic conditions. The associated sleep complaints follow a parallel temporal course. Sleep disturbance associated with anxiety disorders appears to be very common (30). In addition, some patients develop sedative or hypnotic abuse secondary to their anxiety disorder, which can lead to hypnotic-dependent insomnia and complicate the primary disorder.
Somatoform Disorders Associated with Sleep Disturbance
Somatoform disorders include physical symptoms that suggest the presence of a medical condition, but are not fully explained by a medical or physical disorder. In somatization disorder, sleep difficulties and related daytime impairment are common complaints that accompany many of the physical symptoms (e.g., pain or gastrointestinal symptoms) reported in this disorder. Hypochondriasis, which involves a preoccupation with the idea of having a serious disease based on misinterpretation of bodily symptoms, can also include sleep complaints. Similar to insomnia associated with anxiety disorders, a preoccupation with one’s sleep or the consequences of one’s sleep difficulties can lead to conditioned arousal at bedtime that perpetuates the sleep disturbance.
Psychoses Associated with Sleep Disturbance
Insomnia is a common feature of schizophrenia, schizophreniform disorder, and other functional psychoses. A significant decrease in TST per night may precede psychotic decompensation and accompany the acute exacerbation of psychotic symptoms. Severe sleep disruption can be a significant complication with schizophrenia and lead to suicidal ideation. Acutely ill psychotic patients are more likely to experience severe sleep disturbance, whereas some chronic patients can show almost normal sleep during sleep laboratory testing.
Insomnia Due to Drug or Substance
This category includes insomnia due to the use of prescription medications, recreational drugs, caffeine, alcohol, food (food-allergy insomnia), or exposure to environmental toxins. The use and/or discontinuation of hypnotic medications, stimulants, and alcohol are frequently linked with insomnia.
Hypnotic-dependent Insomnia
Hypnotic-dependent insomnia (31) occurs in association with tolerance to or withdrawal from sedative-hypnotic medications. Several patterns of hypnotic use have been associated with insomnia due to use of sleeping pills. In the first pattern, brief use of a hypnotic, for several consecutive nights, may lead to difficulty sleeping when the drug is stopped (termed rebound insomnia), which may result in resuming use of the hypnotic. In the second pattern, sustained use of hypnotics frequently causes tolerance associated with a decrease in the drug’s hypnotic effects and a return of symptoms. This often leads to an increase in the patient’s dosage. In a third pattern, partial withdrawal may occur when persistent drug tolerance occurs, despite dosage increases, and causes either a generally diminished hypnotic effect or the hypnotic effect to dissipate well before the end of the night. Partial withdrawal can cause a secondary, drug-related sleep disturbance to occur despite continued hypnotic use. Finally, whenever there is abrupt termination of lengthy hypnotic use, severe sleeplessness can occur.
There is a hypothesized pattern of escalating dependence with long-term hypnotic use, as follows. Many patients are hesitant about the use of sleeping pills. They lose confidence and become apprehensive when the initial therapeutic benefits start to decrease. When dosages are increased to offset tolerance, daytime carryover side effects also increase, which may include excessive sleepiness. The daytime symptoms are attributed to the decreased ability to sleep at night. The patient will be distressed and may become focused on the perceived need for more effective medication. The patient may consult new physicians and try varied sedative—hypnotic compounds.
Finally, if the hypnotic therapy is stopped, sleep will return to the predrug pattern. After stopping hypnotics, the subjective quality of sleep is often judged to be worse than before starting the medication. The patient may fear that the ability to sleep normally has been permanently lost. There may be central nervous system (CNS) withdrawal symptoms, which can include nausea, aches, irritability, and restlessness. The experience of withdrawal symptoms can predispose the patient toward resumption of chronic hypnotic use, in search of more normal sleep and improved daytime functioning. As an important complication, anxiety, nervousness, or depression may result from a hypnotic-dependent sleep disorder, especially during withdrawal.
After hypnotic withdrawal, sleep may gradually normalize. More often, sleep disturbance will persist, and it will be important to seek to determine etiology. There could be a chronic psychophysiological insomnia or insomnia due to mental disorder. PSG may be indicated to assess for apnea, PLMD, and other physiologic sleep disorders.
Stimulant-dependent Insomnia
The stimulant-dependent sleep disturbance is characterized by reduction of sleepiness or suppression of sleep by CNS stimulants. When the drugs are withdrawn, sleepiness and sleep increase. Stimulant-dependent insomnia generally applies to the abuse of stimulants. Stimulants that are most commonly associated with sleep problems include caffeine, amphetamines, and cocaine.
When a stimulant is prescribed for medical treatment (e.g., for asthma or attention-deficit/hyperactivity disorder), difficulty falling asleep may occur when treatment is begun, when the dosage is increased, or the administration times are moved closer to bedtime. The difficulty usually ends after treatment changes become more established. Stopping use of a prescribed stimulant may also cause transient withdrawal symptoms, such as daytime sleepiness.
When stimulants (e.g., caffeine) are used to suppress sleep or to maintain a drug-mediated sense of well-being, sleep problems occur. Drug tolerance develops, and this causes dosages to escalate. Inevitably, periods of high-dosage use will lead to exhaustion and periods of somnolence.
Psychiatric symptoms are prominent in association with chronic stimulant abuse. During drug administration, the symptoms may mimic paranoid schizophrenia. Because intravenous stimulant administration is common, infectious diseases may be a complication.
A mild case of stimulant abuse could be misdiagnosed as sleep-onset insomnia due to anxiety disorder. When stimulant abuse is chronic, the differential includes schizophrenia or mania.
Alcohol-dependent Insomnia
Alcohol is commonly used as a sleep aid since the immediate effects from a dose of alcohol include sedation. Sleep laboratory recordings show that alcohol consumed near bedtime will promote sleep during the first 4 hours in bed, but will subsequently lead to increased wakefulness during the last 2 to 3 hours of an 8-hour sleep period. In addition to promoting sleep onset at bedtime, the sedative effects of alcohol can also increase snoring and obstructive sleep apnea (OSA). During the daytime, even a small dose of alcohol ingested by a sleepy individual can increase the risk for automobile accidents.
The long-term effects of alcohol upon sleep and daytime functioning are complex and change over time. The distribution of nocturnal sleep stages varies from person to person, and distribution can vary based on the duration and amount of alcohol use.
The alcohol-dependent sleep disorder is characterized by regular ingestion of ethanol in the evening as a hypnotic. There may be an underlying disorder that causes sleep-onset insomnia, which the patient chooses to self-medicate with alcohol. In a representative case, alcohol ingestion begins in the evening 3 to 4 hours before bedtime. The patient may regularly consume 6 to 8 drinks. This condition is generally not associated with alcoholism nor the general adjustment problems of alcoholism. Some patients assert that they sleep well as long as they continue nightly alcohol use.
This disorder is rare. It is more frequent after age 40. In suspected cases, there may be an underlying sleep disorder in a person who drinks alcohol in the evening. This would not be diagnosed as alcohol-dependent sleep disorder.
To diagnose alcohol-dependent insomnia, the patient must have taken alcohol as a sleep aid daily for 30 or more nights. The insomnia complaint must have been temporally associated with one or more attempts to discontinue use of alcohol as a hypnotic. The presence of alcoholism must be ruled out, since insomnia is a common consequence of chronic excessive alcohol intake (32)
Insomnia Due to Medical Condition
There are a variety of medical conditions that cause or exacerbate sleep disturbance. Some of the more common disorders include the fibrositis syndrome, sleep-related gastroesophageal reflux, and chronic obstructive pulmonary disease (COPD). Cerebral degenerative disorders, dementia, and parkinsonism are common neurologic conditions associated with insomnia.
Fibrositis Syndrome/Fibromyalgia
This syndrome (33) is characterized by diffuse musculoskeletal pain, chronic fatigue, unrefreshing sleep, and localized areas of increased tenderness in the muscles (tender points). The muscle discomfort complaints generally become stronger during the nighttime.
Fibrositis patients typically complain that their sleep is light, associated with muscle pain and joint stiffness, and they awaken feeling unrefreshed. Tiredness and fatigue persist throughout the day.
This disorder has a chronic relapsing course that can last years. The muscle discomfort and sleep disturbance often lead to anxiety and depression. Sleep complaints may improve with specific treatment, but muscle discomfort may persist. Sleep laboratory testing can help differentiate fibrositis from other causes of unrefreshing sleep. PSG with fibrositis reveals a fairly unique presence of EEG alpha wave activity (8-11 cycles per second) during non-REM sleep. This is especially common during stages 3 and 4, slow-wave sleep, where the combination of alpha and slow waves is referred to as alpha—delta sleep.
The prevalence of the fibrositis syndrome is not known, but apparently is not rare.
Sleep-related Gastroesophageal Reflux
This disorder (34) is characterized by movement of the stomach contents into the esophagus during sleep. When reflux occurs, the patient can awaken with a sour taste, burning sensations, or heartbum-type chest discomfort. The chest pain is usually substernal and is somewhat similar to the pain due to angina. Awakenings associated with this discomfort can lead to an insomnia complaint.
Daily heartburn prevalence is estimated at 7% to 10%. Sleep-related gastroesophageal reflux is a chronic disease that is difficult to cure. It warrants early treatment and preventive measures. Monitoring esophageal pH during sleep can document sleep-related gastroesophageal reflux episodes. The differential diagnosis for sleep-related gastroesophageal reflux includes peptic ulcer and angina.
Chronic Obstructive Pulmonary Disease
COPD is described by a chronic impairment of airflow through the respiratory tract. Sleep disturbance commonly occurs because of COPD and includes difficulty falling asleep, awakenings with respiratory distress, and a feeling of being unrefreshed upon arising from sleep (35). The sleep disturbance is temporally related to the presence of COPD.
The sleep disturbance generally appears correlated with the progression of the underlying pulmonary disorder. As the COPD increases in severity, the sleep disturbance also progresses.
The majority of COPD patients will develop some associated disturbance of sleep quality.
Cerebral Degenerative Disorders
The cerebral degenerative disorders are slowly progressive conditions characterized by abnormal behaviors or involuntary movements, such as Huntington’s disease, spastic torticollis, and blepharospasm. These disorders can produce insomnia. Sleep symptoms include insomnia, EDS, and abnormal motor activity. The circadian sleep-wake cycle may also be disturbed. Sleep disturbance increases with the progression of the disease.
PSG may be indicated if there is a clinical need to rule out other movement disorders that are not associated with cerebral degeneration, such as PLMD and REM sleep behaviour disorder (RBD).
Dementia
Dementia refers to a deterioration of intellectual capacity due to a chronic, progressive degenerative disease of the CNS. The sleep disturbance in dementia is characterized by delirium, agitation, combativeness, and wandering (36). Sleep is fragmented, with frequent awakenings; often there is difficulty falling asleep at bedtime and early final awakening.
Sleep and nocturnal cognitive abilities may be particularly disturbed in demented patients; often the nighttime hours present the most difficult management challenge for caregivers. Sleep disturbance that is characterized by wandering and confusion is often summarized as the sundowner syndrome, and the syndrome is exacerbated by physical illness or hospitalization. The sleep disturbance follows the course of the dementia. Nocturnal symptoms and sleep disturbance are often the cause for institutionalization.
The prevalence of sleep disturbance among all patients with dementia is not known, but it is common. The prevalence of severe dementia is estimated to be 5% to 15% of institutionalized patients older than age 65.
Parkinsonism
Parkinsonism refers to a group of neurologic disorders with hypokinesia, tremor, and muscular rigidity. Insomnia is the most common sleep-related complaint in patients with parkinsonism, although a variety of sleep-related symptoms are common.
There is no typical sleep pattern revealed by PSG. The following features are commonly observed: (a) long sleep latency, sleep fragmentation, and reduced REM sleep; (b) tremor usually stops during sound sleep, but may reappear with arousals; (c) bradykinesia and rigidity that are associated with decreased ability to get out of bed and reduced ability to change position; (d) abnormal movements, including PLMs and isolated twitches; and (e) respiratory abnormalities (including apneas and hypoventilation).
Medications for parkinsonism can improve sleep disturbance by decreasing rigidity, but conversely may exacerbate sleep disturbance and can cause new sleep complaints. Sleep complaints generally worsen as the disorder progresses and the duration of treatment lengthens.
Parkinson’s disease affects approximately 0.2% of the general population. The prevalence increases with age. Onset is commonly between ages 50 and 60. Among people who seek treatment for parkinsonism, 60% to 90% have sleep complaints.
Insomnia Associated with Circadian Rhythm Disorders
The major feature of circadian rhythm disorders is misalignment between the patient’s sleep pattern and the desired time of day for sleeping. The patient is unable to sleep when sleep is desired and needed. As a consequence, periods of wakefulness may also occur at undesired times.
Delayed Sleep-phase Syndrome
The delayed sleep-phase syndrome (DSPS) (37) has the daily major sleep episode delayed, or shifted to a later time period, in relation to the desired clock time. This shift of the sleep period causes symptoms of sleep-onset insomnia and, in the morning, difficulty awakening and difficulty arising at the desired time. When not compelled to sleep on a strict schedule, such as on weekends, the patient experiences normal sleep quantity and quality, but at a delayed clock time relative to the patient’s usual earlier sleep schedule.
Several additional features are basic characteristics of DSPS: (a) sleep-onset and wake-up times seem intractably later than desired and unresponsive to enforcement of a strict sleep schedule, (b) patient reports normal ability to stay asleep once sleep has begun, and (c) severe difficulty awakening at the patient’s desired time for arising in the morning.
In relatively pure cases of DSPS, a carefully completed daily sleep log shows the pattern. In cases complicated by alcohol, sleeping pills, or mental disorders, the sleep logs may also show frequent awakenings during the delayed sleep periods, which reflect the additional factors. When DSPS occurs in the context of severe psychopathology, sedative abuse, or alcohol abuse, it is often unresponsive to standard treatment with behavior therapy techniques until those factors are dealt with.
This disorder is estimated to affect 5% to 10% of patients with insomnia complaints who are seen at sleep disorders centers.
Advanced Sleep-phase Syndrome
In this disorder (38), the daily major sleep episode is advanced (shifted to an earlier time period), in relation to the desired clock times for retiring and arising. The advanced phase results in strong early evening sleepiness, falling asleep early, and a final awakening that is correspondingly earlier than desired.
There is intractable and chronic inability to delay the beginning of early evening sleep and inability to continue sleep past an early morning final awakening. There are negative social consequences because evening activities are often missed.
This disorder is not often diagnosed and it is apparently rare. Many research studies have shown a mild advance in sleep phase among elderly individuals. Theoretically, this could make elderly individuals at increased risk for advanced sleep-phase syndrome (ASPS).
The early morning awakenings of depression must be differentiated from ASPS. Depression is usually accompanied by other sleep symptoms (e.g., frequent awakenings and unique abnormalities of REM sleep). PSG can help differentiate the patient’s sleep pattern from the depression pattern.
Shift-work Sleep Disorder
A shift-work sleep disorder (39) consists of transient symptoms of insomnia and excessive sleepiness that recur in relation to work schedule.
A shift-work sleep complaint typically affects a third shift (night shift) employee with inability to sleep for a normal length of time, when the major sleep period is begun in the morning (e.g., at 6-8 AM). TST during the daytime sleep period is often reduced by 1 to 4 hours. Early morning shift workers and evening shift individuals can also have shift work-related difficulty sleeping. The disorder also includes excessive sleepiness during work shifts (mainly on the night shift).
Only gold members can continue reading. Log In or Register to continue