Fig. 8.1
Typical anatomic landmarks around the foramen of Monro – choroid plexus (cp), thalamostriate vein (tv), fornix (f)
“Learning by doing” can have fatal consequences because the possibility to manage intraoperative complications such as haemorrhage using the endoscope is limited. This means that an optimal targeting is essential without harming delicate structures.
8.3 Endoscopes
Various rigid and flexible, steerable endoscopes (encephaloscopes, ventriculoscopes and spinaloscopes) are available [10]. The specifications vary according to the planned operative application. The optimal neuroendoscope has not yet been developed. It should have the flexibility and the steerability of fibrescopes, combined with the optic resolution of Hopkins optics and optimal light transmission. Furthermore, it needs the integration of two or more working channels for bimanual preparation and the option for adaption to modern neuronavigation systems. The advantage of the rigid lens scope is the brilliant and bright optical quality; however, the working space is limited due to the straight predetermined trajectory. The field of action can be enlarged by the use of different angled optics, which vary from 5° to 120°, depending on the endoscopic system. These angled endoscopes can also be used during endoscopy-assisted microsurgical interventions, such as cerebellopontine angle surgery, pituitary surgery or aneurysm surgery.
Despite a lower optical quality, flexible endoscopes offer the opportunity to “look around corners” and have a high degree of manoeuvrability, especially in the ventricular system. Ultrathin flexible endoscopes can be used as “baby” endoscopes through larger endoscope working channels.
A new and very sophisticated technique, which will become available in the future, will integrate the third dimension into neuroendoscopes. We have tested several prototypes of rigid and flexible 3D endoscopes with Hopkins optics. These endoscopes give a high quality of field of depth and will provide a higher level of accuracy for neuroendoscopic interventions.
As a result of the long experience with different neuroendoscopes, we designed a new ventriculoscope. The ventriculoscope has a working length of 180 mm. The outer diameter is 6.5 mm. The direction of view is 5°. There are three channels, one for instrumentation (2.8 mm), one for suction (1.4 mm) and one for irrigation (1.4 mm) (Fig. 8.2).
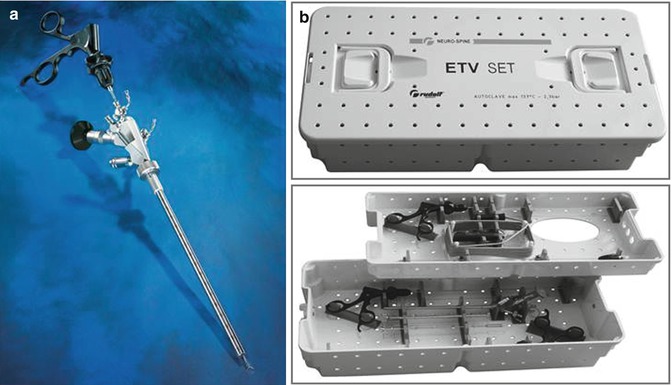
Fig. 8.2
(a) Multipurpose ventriculoscope according to Hellwig and (b) ETV-SET (Rudolf Medical Co.)
8.4 Fixation and Guiding Systems
To avoid uncontrolled movements during neuroendoscopic procedures and to free the endoscopist from fatigue, different fixation devices have been developed and are available. The Marburg neuroendoscopy fixation and guiding system consists of a retaining arm with joints, which allows movements of the instrument in all spatial directions. It provides the necessary stability to the whole endoscopic system during the operative procedure. The working depth is regulated by micrometre screws. The system is compatible to various stereotactic and microsurgical holding devices [20].
8.5 Video Camera System
Different light sources and camera systems are available with the newly developed charge couple device (CCD) technology. We use the Monolith Line ® Video Camera System with extremely light-sensitive 3xHD 1/3″ CCD sensors. The camera head has special features: 2× multifunctional remote buttons preconfigured for simultaneous control up to six special camera functions directly via camera head, standard c-mount connector and a high-quality optical zoom coupler (f = 21–36 mm). The camera control unit has a full HDTV resolution of 1920–1080 pixel, 10× user application presets – 3 of these user settings are in addition individually programmable, excellent visual characteristics and a high-contrast colour reproduction.
8.6 Picture Distribution and Video Transmission System
The 44 HD SDI OR–MATRIX ® is, due to its function range, picture distribution from one or more OR camera systems to various diagnosis, monitoring or operation monitors respectively documentation systems, which may be operated separately or simultaneously, as well as real-time transmission of surgical interventions through an enabled LAN network (e.g. intranet), a useful additional equipment for each operation room used for minimally invasive or open surgery. It combines high-definition video routing in full HDTV resolution of 1920 × 1080 pixel, system oriented, throughout continuous HD signal chain; latest H.264-based video transmission via LAN; programming and storage of video routes; live transmission from the operating theatre via LAN; and an IT-based solution for interactive consultation.
8.7 Documentation System
The Monolith Line HDTV Documentation System (1080 HD SDI Controltec®) meets the demands for a simple yet comprehensive documentation of the course of operations, both of open and minimally invasive surgeries, and it is also a solution based on the latest imaging and data storage. The features of this system are based on a consequent implementation of a consistent HD video chain. It uses digital video signals only, which provide a complete HDTV resolution. The information storage is in HDTV format. Consistent picture quality with a resolution of 1080 TV lines from the source or pictures up to their recording and saving is guaranteed. There are optional extension tools like network functioning. Figure 8.3 shows all the components of the Monolith Line System.
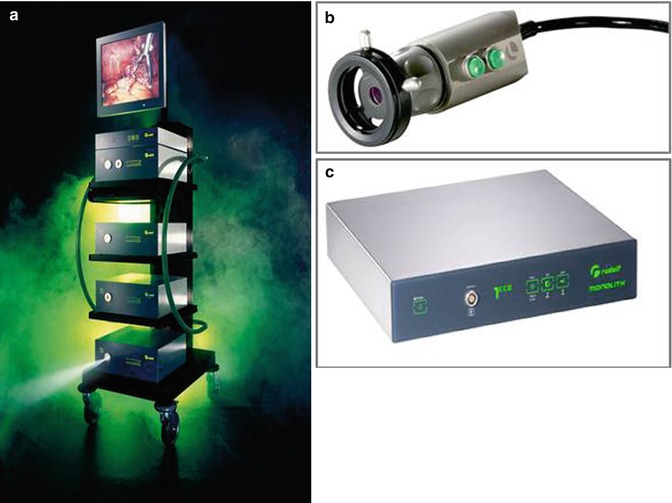
Fig. 8.3
(a) Complete Monolith Line System, (b) camera head, (c) camera control unit
8.8 Supplementary Instruments
Moving endoscopes and instrumentation within preformed spaces through small working channels demands training. The working instruments enter the viewing field at the tip of the endoscope anteriorly, posteriorly or laterally. It may be difficult to watch the instruments; if the endoscope is too close to the target area, injury of brain tissue is possible. It is advisable to have a safe distance of 5 mm, when the working instrument enters the region of interest.
A variety of supplementary working instruments for neuroendoscopic interventions are now available (Fig. 8.4).
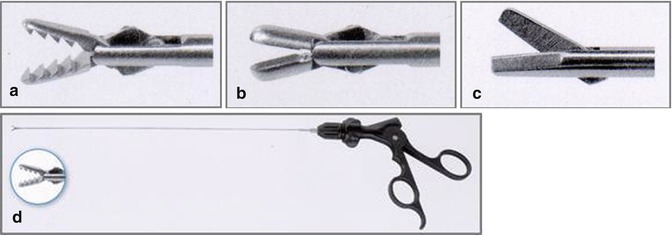
Fig. 8.4
(a) Grasping forceps, (b) biopsy forceps and (c) microscissors with diameters from 1.6 for ETV, tumour biopsy and dissection of membranes and cyst walls. These instruments are detachable and rotatable (d) (Rudolf Medical Co.)
Flexible instruments for fibrescopes have the peculiarity that they do not open gradually. They snap with a short delay between the action of the hand and the effect at the tip of the instrument. This is different from the action of rigid instruments and also needs familiarisation.
8.9 Electrosurgery
8.9.1 Electrosurgical Unit (ESU)
Like in microsurgery the further development of electrosurgery contributed to the successful introduction of endoscopy into neurosurgical techniques. Together with the technical development and increasingly frequent use, there has been demand for more precise instruments and generators [17]. The technical problem has been the regulation of the cutting depth, cutting speed, electrode size and cutting quality of differing tissues. In practice, this often meant that an insufficiently low-power setting would deliver a less desirable cut and a rather mechanical “pulling up” of the tissue. This led to the use of a higher output power in order to ensure a safe cut. When a superficial cut was then made, the electrical voltage was too high, i.e. the applied power was too high for cut. The consequence was either carbonisation during incision or after cut, or the tip of the fine instrument could burn out.
An insufficient power setting for coagulation could result in insufficient haemostasis; a power setting that was too high resulted in the electrode sticking to the tissue, which could also lead to bleeding, when the electrode was removed. Another unintended effect was that carbonisation could occur. These problems were solved by the development of an automatically controlled electrosurgical unit (ESU) and precise instruments made of novel materials. Thus, for the first time, it was possible to achieve reproducible cutting and coagulation qualities even using differing instruments. Modern microprocessor-controlled solid-state bipolar coagulating and cutting systems contribute significantly to the performance of major microsurgical and neuroendoscopical procedures, decreasing operative time and blood loss whilst facilitating outcome.
Recently an automatically controlled generator was designed where the output voltage and spark intensity remain constant, forming the basis for reproducible cut. According to the latest research, voltage regulation in neurosurgery is more relevant than spark regulation. Voltages can be preselected within a useful range, i.e. no voltages below 200 V can be set which would make it physically impossible to cut, and no excessively strong carbonisation and metallic erosion of the active electrodes can occur. Once the surgeon has preselected his individual setting, the preselected effects will automatically be held constant. By means of such regulation, the cutting quality remains reproducible. Due to the voltage regulation, it is possible to achieve good cutting qualities with a relatively low voltage level. This is the prerequisite to being able to use the finest instruments as described below.
Different principal modes of coagulation are distinguished, of which soft coagulation is an extremely gentle coagulation mode. The electric voltage is relatively low (less than 190 V), so that there is no electric arc between active electrode and tissue. This results in the following advantages: no unintended cutting effect, no carbonisation and significantly reduced sticking effect between active electrode and tissue. These advantages are particularly useful in neurosurgery.
In addition to “the soft coagulation”, there is the function “soft coagulation with auto stop”. In this mode, a sensor measures the optimal coagulation point occurring when intracellular and extracellular liquids are converted to vapour. The generator switches off automatically before carbonisation or sticking of electrodes to the tissue can occur.
In summary, the described electrosurgical unit VIO 300D-2 (Fig. 8.5) provides optimal conditions for neuroendoscopic procedures.

 Current Status and Future Developments of Neuroendoscopic Management of Pituitary Tumours and Craniopharyngiomas
Current Status and Future Developments of Neuroendoscopic Management of Pituitary Tumours and Craniopharyngiomas
 Endoscopy-Assisted Craniosynostosis Surgery
Endoscopy-Assisted Craniosynostosis Surgery
 Neuroendoscopy in Spinal Pathology: Our Experience, New Trends, and Developments
Neuroendoscopy in Spinal Pathology: Our Experience, New Trends, and Developments
 Neuroendoscopic Instruments and Surgical Technique
Neuroendoscopic Instruments and Surgical Technique
 Neuroendoscopic Treatment of Colloid Cysts
Neuroendoscopic Treatment of Colloid Cysts
 Neuroendoscopic Management of Intraparenchymal Lesions
Neuroendoscopic Management of Intraparenchymal Lesions




Related posts:
Current Status and Future Developments of Neuroendoscopic Management of Pituitary Tumours and Craniopharyngiomas
Endoscopy-Assisted Craniosynostosis Surgery
Neuroendoscopy in Spinal Pathology: Our Experience, New Trends, and Developments
Neuroendoscopic Instruments and Surgical Technique
Neuroendoscopic Treatment of Colloid Cysts
Neuroendoscopic Management of Intraparenchymal Lesions
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
