♦ Preoperative
- Medical therapy based on immune status of patient (i.e., AIDS, lymphoma, chronic steroids)
- Most intracranial abscesses require surgical intervention, though some may have initial medical management attempted (better for smaller lesions ≤ 2.5 to 3 cm and early in disease course, when abscess is not yet encapsulated).
- Abscess formed secondary to penetrating injury often requires open débridement
- Previously treated abscesses may be sterile at time of operative culture
- Timing surgical intervention before treatment will increase chances for positive culture results
- Approach based on location of lesion(s) (Fig. 74.1)
- Superficial: open treatment preferred
- Deep: stereotactic aspiration preferred
- Ventricular: may require aspiration along with intrathecal antimicrobial therapy
- Superficial: open treatment preferred
Anesthetic Issues
- Valsalva may increase yield of stereotactic aspiration
- Start antibiotics after cultures obtained when possible
♦ Intraoperative
Stereotactic Aspiration
- Typically performed on a symptomatic deeper mass lesion
- Abscesses in late capsule stage may resist or deflect needle penetration
- Endoscopic aspiration
- May be fewer epileptic complications with stereotactic aspiration rather than open excision
< div class='tao-gold-member'>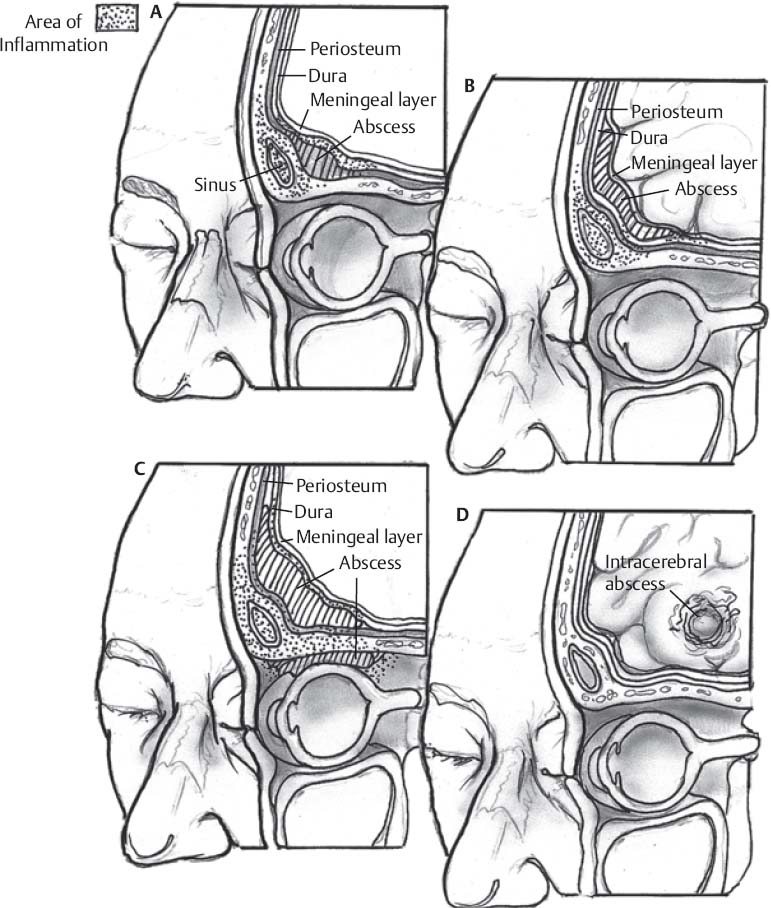 Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


