Chapter 13 Intracranial Aneurysms
• The incidence of intracranial aneurysms is variable throughout the world and is approximately 6% in the international population, with rates being higher in Asian/Finnish populations and those with a high-risk profile. In those patients without any risk factors, the incidence is approximately 2%. Once the aneurysm has ruptured, one third die and two thirds survive, with 50% of survivors leading independent lives.
• The majority of intracranial aneurysms arise at branching points of large arteries. Hemodynamic stress likely contributes to both the initial development and subsequent growth. Aneurysm formation can have many other associated conditions, including autosomal dominant polycystic kidney disease, Ehlers-Danlos syndrome, Loeys-Dietz syndrome, Marfan syndrome, tuberous sclerosis, fibromuscular dysplasia, and other genetic and structural predispositions.
• Approximately 25% to 50% of all patients will have warning symptoms that herald the onset of a major subarachnoid hemorrhage (SAH). The patient’s description of the headache is very important, as most involve “thunderclap” onset or the “worst headache of my life.” Computed tomography (CT) scans detect SAH with high sensitivity. If the scan is negative but suspicion remains high, a lumbar puncture may be performed. Although CT angiography is good for imaging aneurysms greater than 2 mm, cerebral angiography remains the gold standard for intracranial vascular imaging.
• The risk of rebleeding after SAH is greatest on the first day (4.1%). By day 14, the cumulative rebleed incidence is 19%. Once an aneurysm is secure, the most significant cause of morbidity and death is cerebral vasospasm. The onset of cerebral vasospasm begins on day 3 and peaks between 7 and 14 days after SAH. Seventy percent of patients will develop radiographic signs of vasospasm and approximately 30% will develop clinical vasospasm requiring adjunctive therapy.
• The treatment goal of intracranial aneurysms is to exclude them from the parent circulation. In ruptured aneurysms, this must be done so early and safely so that maximum treatment of cerebral vasospasm can be administered if necessary. Symptomatic vasospasm can be treated with triple H therapy (involving hypertension, hypervolemia, and hemodilution) and endovascular means, namely intra-arterial injection of vasodilators or angioplasty.
• To achieve the goal of multidisciplinary cerebrovascular care, aneurysm patients are ideally treated at centers of excellence that employ expertise in all areas of neurovascular care, including endovascular, microvascular, and neurocritical care, and neuroanesthesia.
Intracranial aneurysms are potentially life threatening or disabling vascular lesions, which can pose formidable treatment challenges. Morphologically and pathologically they encompass diverse and occasionally overlapping entities including saccular, fusiform, and dissecting aneurysms with a wide variety of etiological origins, including hemodynamic, traumatic, infectious, and tumorogenic. Although intervention in most cases of ruptured intracranial aneurysms is indicated, the management of unruptured intracranial aneurysms remains controversial. On the other hand, as medicine shifts more toward prevention, greater interest has arisen in defining screening and risk reduction strategies for high-risk populations. Over the last several decades, insight into the pathobiology and pathophysiology has significantly advanced, leading to improvements in the areas of natural history, epidemiology, biology, genetics, therapeutic intervention, and clinical outcomes. This chapter will provide an overview of intracranial aneurysms, clinical presentations, current therapeutic options, and technical aspects of surgical treatment. Although intracranial aneurysms encompass a diverse disease group, as stated earlier, this chapter will focus on the most common type, the so-called “saccular berry aneurysm.”
Epidemiology
The incidence and prevalence of intracranial aneurysms in the general population are very difficult to estimate owing to clustering in various high-risk groups, large numbers of deaths without autopsy or neuroimaging, and the presence of asymptomatic lesions. Furthermore, autopsy studies have demonstrated disparate results that do not appear to link with the prevalence of subarachnoid hemorrhages (SAHs) and rupture risk incidence. Fox1 reviewed the autopsy literature, which spanned from 1926 to 1973, and found the rate of occurrence to be 0.8% when studies included more than 5000 cases and 2% when studies included 2 to 5000 patients. Stehbens2 conducted an autopsy study between 1952 and 1954 and found at least one aneurysm in 5.6% of cadavers. In his review of the pathological literature between 1890 and 1966, the prevalence of aneurysms at autopsy was found to be approximately 2.4% with a range of 0.2% to 9%.3 Intracranial aneurysms in children are rare but are thought to occur in approximately 0.5% to 4.6%.4 Currently, it is thought that approximately 6% of the international population harbor intracranial aneurysms with a higher prevalence in the Asian and Finnish populations (4-9%) and those who harbor significant risk factors, such as environmental, systemic, or genetic.5 Risk factors associated with the presence and rupture of intracranial aneurysms have included high blood pressure, tobacco usage, and genetic- and ethnic-related factors; however, the prevalence of lesions is still thought to be approximately 2% in those without any known risk factors.5 Although the most prevalent risk factors are those that are modifiable, the strongest risk factors are thought to occur through genetic and familial predisposition.
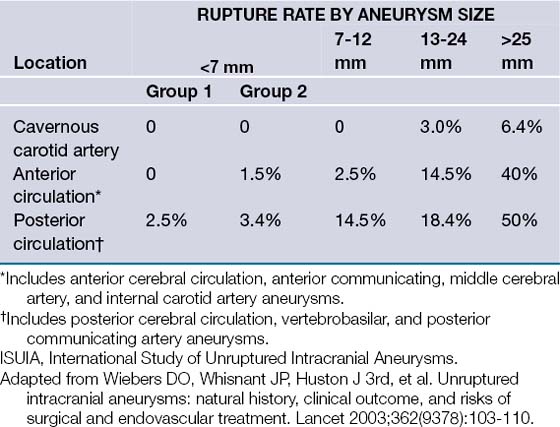
The risk of intracranial aneurysm rupture has also been a controversial topic. Although the annual risk of rupture has been reported to be between 0.1 and 8%,5 depending on variable lesional characteristics, recent prospective data have challenged this view. The International Study of Unruptured Intracranial Aneurysms (ISUIA) reported in two recent publications6,7 that the risk of aneurysm rupture was substantially lower than previously thought, that is, approximately 0% in anterior circulation aneurysms in those less than 7 mm, the most commonly encountered entities (Table 13.1). Although these studies represented the largest prospective collection of data regarding unruptured aneurysms, they have also been met with intense scrutiny and controversy, especially in light of a multitude of studies reporting an order of magnitude greater rupture risk.8 Common problems with estimating the annual rupture risk are the inclusion of all patients with aneurysms, regardless of presentation, proper lesion classification and grouping, taking into account specific lesional characteristics, and proper classification of patients into various risk groups.8 Given the broad spectrum of intracranial aneurysms, a balance of prospective data and clinical experience is necessary to properly and individually assess an individual patient’s rupture risk.
Of those patients who experience (SAH) after aneurysmal rupture, approximately one third return to a functional life, one third live a dependent life, and the last third do not survive.1,5,7,9 As advances in neurocritical care have increased survivability, neurological morbidity rate remains about the same. The greatest risk after the initial aneurysmal rupture is for re-rupture. Once the aneurysm is secure, the greatest risk is of cerebral vasospasm and ischemic complications from such events, thereby underlying the importance of early intervention and close monitoring in the postrupture period.
Pathogenesis
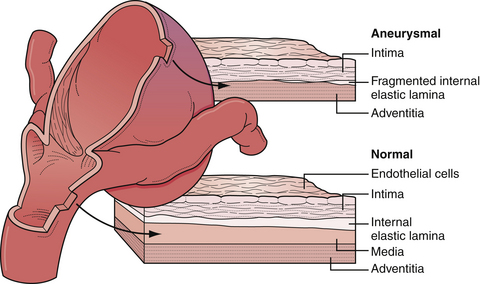
Intracranial arteries are unique to the systemic vascular system in that they lack the external elastic lamina present in extracranial vessels (Fig. 13.1). The pathogenesis of intracranial aneurysms has been thought to be due to a number of congenital factors such as vascular wall defects (i.e., media and elastic lamina), hemodynamic load on tortuous segments and bends with or without branch formation in the appropriate distribution, and discontinuity of the tunica media at origins of small vessels from larger parent vessels. Certainly, a multitude of systemic factors are thought to contribute to aneurysmal pathogenesis, such as degenerative changes, hypertension, atherosclerosis, connective tissue disease, and hemodynamic stress.
Genetic predisposition through various systemic and syndromic conditions has also been associated with the presence of intracranial aneurysms and is thought to represent approximately 10% to 12% of all aneurysms. Autosomal dominant polycystic kidney disease, Ehlers-Danlos syndrome, Loeys-Dietz syndrome, Marfan syndrome, tuberous sclerosis, and fibromuscular dysplasia have all been associated with the presence of intracranial aneurysms.10–15 In recent years, many genetic loci have been proposed to be associated with familial linkage. Ruigrok and associates14 recently reviewed the genetics of intracranial aneurysms and reported that probable loci included chromosomes 5q and 17cen, from which the strongest associations code for versican, an extracellular matrix protein, and TNFRSF13B, a transmembrane activator and a calcium modulator ligand interactor, respectively. Other suggestive loci are 1p34.3-p36.13, 7q11, 19q13.3, and Xp22.9,14,16,17
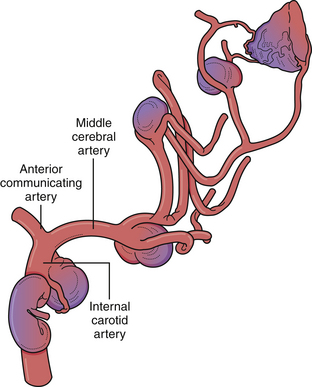
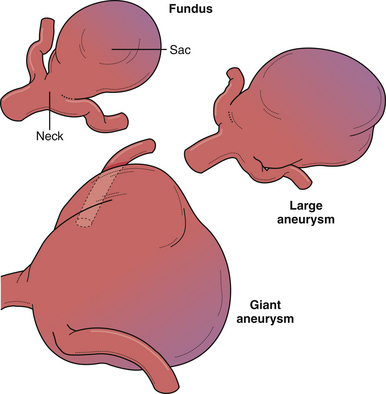
Despite the numerous factors likely to be related to intracranial aneurysm pathogenesis, it is most likely a complex, multifactorial set of circumstances involving anatomical, environmental, and genetic factors that lead to arterial wall weakening and aneurysm formation (Fig. 13.2). In fact, multiple aneurysms are present in up to 30% of patients. However, the majority of lesions are located at branching points along the proximal arterial tree, suggesting that hemodynamic factors play a significant role in aneurysm formation. In addition, formation of de novo aneurysms has been shown to occur at communicating arteries, and fatal rupture of aneurysms has occurred after recruitment of collateral blood flow through communicating arteries after the occlusion of carotid arteries. Furthermore, the incidence of aneurysms associated with high-flow states (e.g., arteriovenous malformations) is higher than in the general population, and some of these lesions regress after treatment of the vascular malformation. Finally, recurrent aneurysms can develop after incomplete treatment, whether by endovascular or microsurgical means.
Natural History
For patients with unruptured intracranial aneurysms, the natural history is much more difficult to resolve. Prior to 1998, the estimated rupture rate for aneurysms was thought to be 1% to 2.5% per year cumulatively. For young patients, the data suggested that intracranial aneurysms should be treated, as the cumulative risk of rupture over many years is very significant. However, the largest and most debated prospective database on unruptured intracranial aneurysms was published in two parts by the International Study of Unruptured Intracranial Aneurysms (ISUIA) and suggested that the rupture risk of unruptured asymptomatic aneurysms was much more benign than once thought (see Table 13.1). The 5-year cumulative rupture rate without a prior history of SAH of anterior circulation aneurysms (not including cavernous carotid or posterior communicating artery aneurysms) was 0%, 2.6%, and 14.5% for aneurysms less than 7 mm, 7 to 12 mm, and 13 to 24 mm, respectively, and it was 2.5%, 14.5%, and 18.4%, respectively, for the same three size groups of aneurysms in the posterior circulation (including posterior communicating artery aneurysms). Patients with a history of SAH with aneurysms less than 7 mm had a 1.5% rupture rate over 5 years with further increases in rates with increasing aneurysmal size. Many limitations of the ISUIA study have been reported. Selection bias likely played a substantial role because patients with aneurysms that were thought to be at a high risk of rupture, namely, those with multiple lobulations, hemodynamic factors, and so on, were treated and therefore were not included as part of the study. Further, cavernous carotid aneurysms were included in these studies, but these aneurysmal lesions rarely result in SAH. Lastly, the annual incidence of SAH in the United States is approximately 30,000, which when calculated against the incidence of aneurysms, results in a rupture rate of at least 1% per year, significantly higher than that calculated in the ISUIA study.18,19
Other morphological factors of aneurysms, besides the size of the aneurysmal dome, have been thought to contribute to the annual rupture risk. More specifically, neck width, dome width, aneurysm shape, aspect ratio (height/neck width), and bottleneck factor (dome width/neck width) have been examined.8 Among these, a higher aspect ratio (>1.6) is thought to be associated with an increased rupture risk. Other morphological characteristics, such as lobulations, daughter sacs, and surface irregularity, have long been associated with higher rupture risk8 (Box 13.1). Finally, the hemodynamics of the surrounding vasculature to an unruptured aneurysm may put a particular lesion at a greater risk of rupture, for example, dominant A1 feeding into an anterior communicating artery aneurysm.20
Clinical Presentation
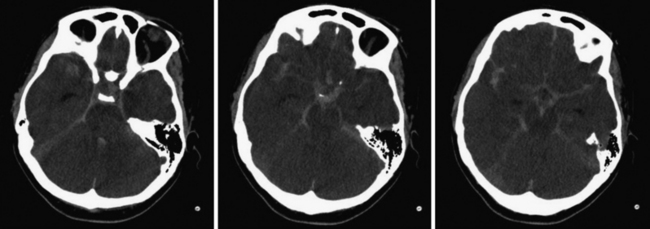
For patients who present with frank aneurysm rupture, the most common clinical symptoms and signs are the sudden onset of the worst headache of their life, severe nausea and vomiting, altered mental status, nuchal rigidity, and loss of consciousness. Most emergency departments automatically order a head computed tomography (CT) scan without contrast to evaluate these patients for possible SAH, although misdiagnosis remains a major problem (Fig. 13.3). It is of paramount importance to identify these patients because aneurysmal re-rupture has devastating consequences. With the technological advancements of CT scanners, the sensitivity/specificity of SAH detection is greater than 98% in the first 2 days.21 As such, lumbar puncture is not necessarily indicated unless the insinuating event happened at least 3 days prior or if head CT image is negative despite strong clinical suspicion. A lumbar puncture is used to detect evidence of red blood cells and xanthochromia. After confirmation of SAH on CT scan, a CT angiogram (CTA) is performed, especially if the clinical history is highly suggestive of aneurymal SAH. CTA detection of intracranial aneurysms is now on the order of 99% for aneurysms larger than 2 mm.22,23 Digital subtraction angiography (DSA) is now often reserved at our center for the absence of or questionable intracranial lesions seen on CTA or when the clinical picture favors endovascular intervention.
Approximately 25% of patients who present with SAH have had sentinel headaches (same symptoms as those related to SAH) in the weeks prior to presentation. The diagnosis of “sentinel headache” is only made in retrospect if the patient did not seek medical attention or was misdiagnosed recently when evaluated. These “sentinel headaches” are thought to be due to “minor leaks” or acute aneurysm expansion. Education of both the public and the medical community (especially physicians from primary care, neurology and emergency medicine) could go a long way to earlier diagnosis and improvement of outcomes. Any sudden onset thunderclap headache should be assumed related to an intracranial aneurysm until proved otherwise.
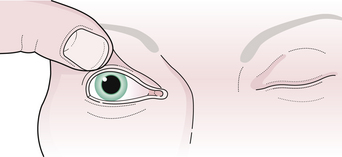
Various neurological deficits can be detected in aneurysm patients due to local mass effect, increased intracranial pressure, or thromboembolic complications from progressive thrombosis of a large or giant aneurysm. Common neurological findings include third cranial nerve palsy, visual loss (afferent pupillary defect), trigeminal symptoms, sixth cranial nerve palsy, nystagmus, vertigo, persistent nausea, and altered mental status (Fig. 13.4). These symptoms can occur from progressive enlargement of an unruptured aneurysm (Fig. 13.5). Focal neurological deficits can occur with embolization of clot from a thrombotic aneurysm. Magnetic resonance imaging (MRI) may be indicated in the workup of neurological findings but should not overlook the possibility of either aneurysms or the presence of subarachnoid blood.
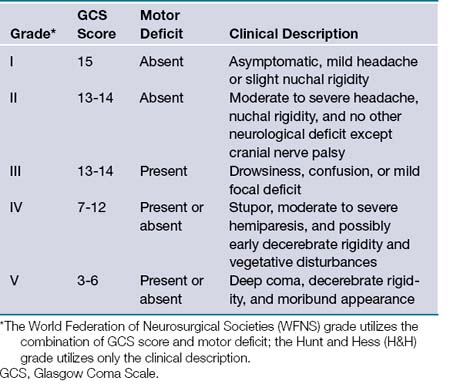
Once aneurysmal SAH has been confirmed, the initial neurological examination is important in determining prognosis. A variety of grading scales have been developed, most commonly the World Federation of Neurosurgical Societies (WFNS) and Hunt-Hess grading scales (Table 13.2). Morbidity and mortality rates increase with a higher grade in each scale.
Initial treatment for SAH involves a complete medical evaluation. Some patients can present with acute mental status changes that are the result of hydrocephalus. In these cases, an extraventricular drain should be placed not only to relieve the hydrocephalus but also to monitor the intracranial pressure. Permanent cerebrospinal fluid (CSF) diversion is necessary in approximately 10% of patients, owing to the hematoma breakdown products affecting the functioning of the arachnoid granulations. However, the most common medical complication after SAH is cerebral ischemia secondary to cerebral vasospasm. Vasospasm usually starts by the fifth posthemorrhage day and can be a threat for up to 14 days after hemorrhage. Angiographic vasospasm has been shown in up to 70% of patients, whereas symptomatic clinical vasospasm occurs in only about 30% of patients.24–26 Medications often administered to SAH patients, namely nimodipine, a calcium channel blocker, and pravachol, an HMG CoA (3-hydroxy-3-methylglutaryl coenzyme A) reductase inhibitor, are thought to limit, although not prevent, the onset of symptomatic vasospasm, thereby improving outcomes, not incidence.27 However, controversy still exists regarding the absolute effects of these medications.
Subarachnoid Hemorrhage
Medical Complications with Subarachnoid Hemorrhage
Subarachnoid hemorrhage has potentially devastating effects not only on the brain but also on the other organ systems of the body, both in the acute and chronic phases after aneurysmal rupture. Although it is beyond the scope of this chapter to detail every medical complication that can occur, brief mention will be made of the most commonly encountered medical complications (Box 13.2).
Soon after the event of SAH, a generalized sympathetic response is often encountered, which has profound effects on the cardiopulmonary system as well as the systemic vasculature. The massive surge of catecholamines after SAH likely induces various degrees of cardiac injury, as evidenced by increased serum troponin T levels, electrocardiogram (ECG) changes, and sometimes severe cardiac wall motion abnormalities.28–31 Pulmonary complications are also anticipated after SAH. Pulmonary edema can occur after SAH and is usually secondary to cardiac failure from cardiogenic shock.28,30 However, acute respiratory distress syndrome (ARDS) can result from primary pulmonary tissue damage from the initial sympathetic response. Further, in patients who lose consciousness after SAH, evidence of aspiration pneumonitis has been reported, which can develop into pneumonia or ARDS.32 When patients are dependent on mechanical ventilators after SAH, an increased incidence of pneumonia occurs.32
Electrolyte disturbances are anticipated after aneurysmal SAH. The most common electrolyte abnormality after SAH is hyponatremia, which occurs in approximately one third of patients.33 Owing to the endocrine disturbances of sodium and intravascular volume regulation, excessive renal excretion of sodium and dehydration lead to a condition known as cerebral salt wasting. In patients with lethal hemorrhages or aneurysms associated with hypothalamic tissue or vascular supply to such tissue, diabetes insipidus can occur, and leads to progressive hypernatremia and increasing urine output. In rare cases, SAH can lead to acute renal failure through posterior hypothalamic dysregulation, which may trigger renal vasoconstriction by activation of the renin-angiotensin system and thereby can reduce renal blood flow.34
Infectious complications also can accompany SAH patients in the chronic phases. Patients who are on mechanical ventilators, arterial and venous access lines, bladder catheters, and ventricular drains are always at an increased risk of infection. Appropriate changing of intravascular lines, tracheostomy procedures, timely removal of ventricular catheters, and changing of bladder catheters is thought to reduce the overall risk of infections.35
Finally, neurosurgical patients are known to experience a higher risk of developing deep venous thrombosis (DVT), potentially leading to an increased incidence of venous thrombosis and even thromboemboli.36 Most medical centers currently use compression stockings and pneumatic compression devices to reduce the incidence of DVT and pulmonary embolism (PE). In patients who develop DVTs and are not able to be anticoagulated due to recent SAH, vena cava filters are often placed. Early administration of prophylactic low-molecular-weight heparins is often used in SAH patients 48 to 72 hours after admission to decrease the risks of DVT/PEs (after aneurysm is secured).
Treatment of Subarachnoid Hemorrhage
Systemic circumstances (e.g., cardiopulmonary instability) may prevent a patient from being ready for aneurysm treatment. Therefore, antifibrinolytic therapy has been suggested to aid in reducing the risk of re-bleeding. The Cooperative Aneurysm Study found that the re-bleeding rate at 14 days was 11.7% if antifibrinolytics were used and 19.4% if no antifibrinolytics were used.37 However, in the face of vasospasm, the risk of ischemic events is higher in patients in whom antifibrinolytics were used, thus equalizing the mortality rates between the two groups. As such, we tend to use antifibrinolytics in patients who present in poor grade or who are medically unstable for treatment with the knowledge that ischemic complications are possible and CSF diversion may be necessary.
Symptomatic vasospasm is the leading cause of morbidity and death following aneurysmal SAH.25,26 Treatment for vasospasm has evolved over the past decade but still lacks definitive treatment (Fig. 13.6). Patients require diligent monitoring and treatment for up to 14 days after hemorrhage through invasive blood pressure monitoring, cerebral blood flow monitoring (transcranial ultrasound, CT/MRI perfusion studies), and often aggressive medical therapy including hypertensive and hypervolemic therapy and hemodilution (triple H therapy). In symptomatic patients, endovascular therapy can also be employed, which may involve intra-arterial injection of vasodilators or balloon angioplasty. In addition to spasm in the large conducting vessels, the phenomenon of SAH also triggers more complex events, which can lead to patchy infarcts in areas apparently unaffected by angiographically visible vasospasm.

FIGURE 13.6 Prophylactic and therapeutic strategy for vasopasm at Northwestern University Medical School.
Much study has been invested in pharmacological prevention of arterial narrowing but research has not demonstrated changes in the long-term outcome of patients treated with such agents. Calcium channel blockers (e.g., nimodipine) have been used since the 1980s but have produced modest results in the literature.38–41 More specific pharmacological agents, namely, selective endothelin 1a receptor antagonists, have shown promise in effectively preventing and reducing arterial narrowing but failed to demonstrate any effect in long-term outcomes.25,26 Lastly, it has been suggested that statin therapy in conjunction with calcium channel blockers may lower the incidence of delayed cerebral ischemic events and improve patient outcomes; this was demonstrated in a phase II study.42 However, a recent meta-analysis of the literature claims that no statistical benefit could be gleaned from the literature. Nevertheless, many institutions now initiate acute therapy with both calcium channel blockers and statins.43
Approximately 70% of patients demonstrated some form of radiographic arterial narrowing, which does not necessarily warrant immediate treatment. However, up to 30% of these individuals will progress to have clinically symptomatic vasospasm, warranting immediate evaluation and treatment, medical or otherwise. Monitoring vasospasm in comatose patients becomes problematic because of the absence of a clinical examination to follow, thereby placing emphasis on indirect evidence such as transcranial Doppler or CT/MRI perfusion studies on progressively worsening cerebral blood flow changes to indicate time of potential treatment. Medical management of vasospasm has traditionally been through “triple H” therapy, involving hemodilution, hypertension, and hypervolemia.26,30,38,41 Maximizing the rheological properties of blood (i.e., maintaining a hematocrit level from 30 to 34) improves tissue perfusion. Should a focal neurological deficit develop, we immediately raise the systolic blood pressure up to the 175 to 200 mm Hg range or until the deficit reverses. In addition, we will volume expand and raise the central venous pressure (CVP) of the patient to the 10 to 15 mm Hg range. If these medical maneuvers do not result in an improvement of the patient’s condition and a surveillance CT scan does not demonstrate any areas of obvious infarction, we then proceed immediately to the angiography suite for a diagnostic angiogram and potential intra-arterial therapy.
Hydrocephalus, either communicating or noncommunicating, frequently develops in the first few days after SAH and partly explains the appearance of a globally edematous brain. Upon recognition that symptomatic hydrocephalus exists, it is suggested that CSF diversion be performed, usually by placement of an extraventricular drain (EVD). Careful placement of an EVD and conservative drainage of CSF must be maintained to avoid the possibility of an acute increase in the transmural pressure across the aneurysm or ventricular shift leading to the destabilization of the tamponading aneurysmal clot. In about 10% of patients, permanent CSF diversion is necessary.44 The risk of permanent hydrocephalus is higher in patients with ruptured upper basilar trunk aneurysms.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


