Intracranial pressure
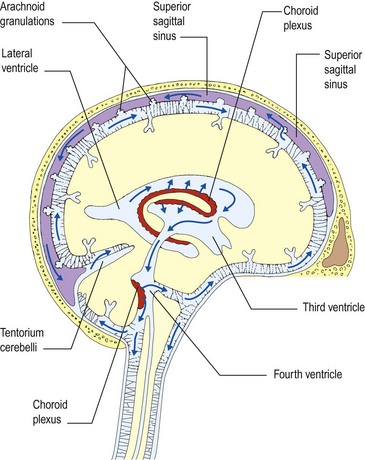
Before considering coma and unconsciousness it is useful to understand intracranial pressure and brain herniation. The intracranial compartment is a fixed box containing brain, blood and CSF. The dynamics of CSF flow are illustrated in Figure 1. Pressure may be increased by:



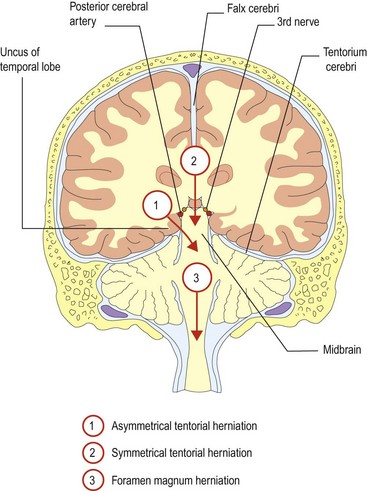
There are two semi-rigid sheets, the falx cerebri and the tentorium cerebelli, which almost divide the brain into separate compartments with relatively small apertures between them (Fig. 2). When the pressure rises in one compartment, the brain may herniate through the apertures into adjacent compartments. The cerebellar tonsils and fourth ventricle may also be forced down through the foramen magnum. These are life-threatening complications that further block CSF flow, causing a vicious circle of rising intracranial pressure, resulting in coma (see below).
In some circumstances, such as idiopathic intracranial hypertension (IIH), previously called benign intracranial hypertension (BIH), no cause may be found (p. 40).




