32 Intracranial Venous Revascularization
Introduction
Ignoring the cerebral venous system (CVS) during surgery would entail disastrous consequences; therefore, thorough knowledge of venous anatomy and physiology is of prime importance in intracranial neurosurgery.1–8
The “dangerous” venous structures
The Dural Venous Sinuses
The superior sagittal sinus (SSS), a major dural sinus, has three parts. The anterior third receives the prefrontal afferent veins (Figure 32–1). It is generally admitted that its sacrifice is well tolerated. Actually, severe mental disorders, personality changes, or loss of recent memory with a general slowing of thought processes and activity, or even akinetic mutism, may occur if sacrificed. The mid-third receives the voluminous cortical veins of the central group. Interruption of this portion entails high risks of (bilateral) hemiplegia and akinesia. The posterior third, as well as the torcular Herophili, which receives the straight sinus, drains a considerable amount of blood. Interruption would inevitably provoke potentially fatal intracranial hypertension.
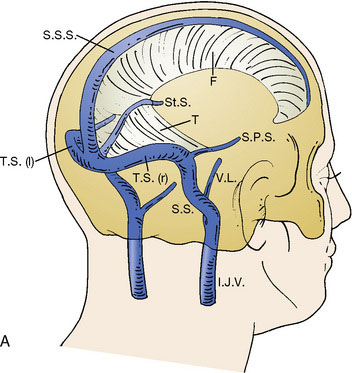
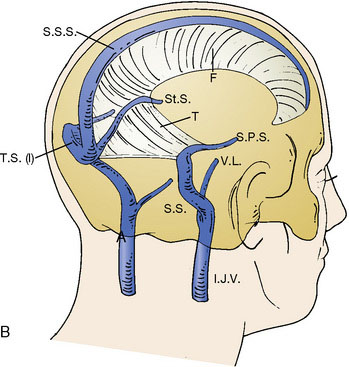
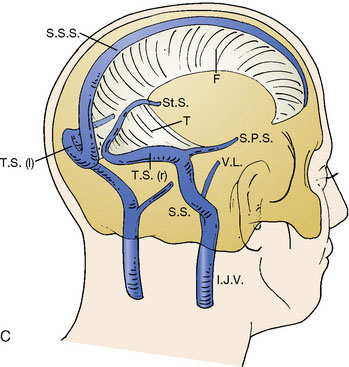
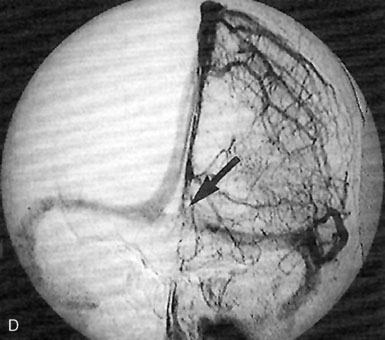
All of these anatomical configurations have surgical implications and must be taken into account before considering interrupting sinuses.9–11
The Deep Veins of the Brain
The deep veins of the brain drain toward the venous confluent of Galen (Figure 32–2). The term venous confluent is appropriate since, in addition to the two internal cerebral veins, the Galenic system receives the two basilar veins of Rosenthal, and also veins from the corpus callosum, the cerebellum (mainly the vermian precentral vein), and the occipital cortex.
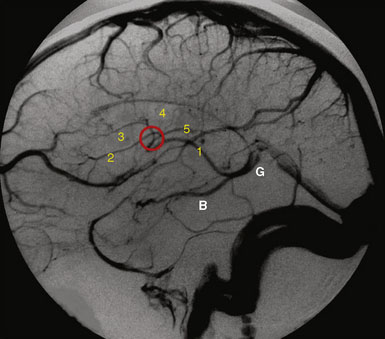
Regarding the precentral vermian vein, it is generally accepted, and we agree, that its sacrifice to approach the pineal region is without danger.1–3
The Superficial Veins
Any of the superficial veins of a certain caliber presumably have a functional role. The superficial veins belong to three “systems”: the midline afferents to the SSS, the inferior cerebral afferents to the TS, and the superficial sylvian afferents to the cavernous sinus (Figure 32–3). These three systems are strongly interconnected, but there is considerable variability among patients. The main anastomotic veins are Trolard to the SSS, Labbé to the TS, and great superficial sylvian, all of them bearing important surgical implications.
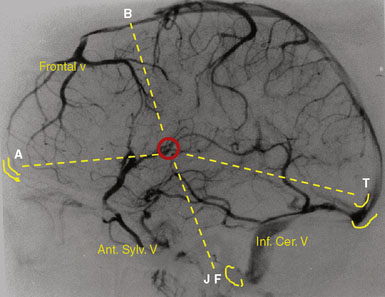
Intracranial approaches, especially skull base ones, must be prepared taking into account the organization of the superficial venous system (see Figure 32–3).7,13,14
Veins of the Posterior Fossa
Sacrifice would expose the cerebellum to swelling or infarction. The conventional statement that the superior petrosal vein, especially when voluminous, can be interrupted without danger needs to be reconsidered. Our experience is that this venous complex should be respected.1
Avoidance of venous occlusions during surgery
The role played by venous occlusions during surgery in the occurrence of postoperative hemorrhagic infarcts is undeniable.1–3,7 Retraction of the brain provokes local congestion by compressing the cortical venous network, reduction in venous flow by stretching the bridging veins, and thrombosis of veins if compression of the retractor is prolonged.15 Excessive brain retraction can be avoided by specially designed approaches and limited opening of the dura, obeying two principles, including the minimally invasive opening and bone removal associated with craniotomy at the base of the skull. Keyhole approaches or limited opening of the dura prevent excessive retraction and consequently avulsing veins.
A bridge vein acting as a limitation may occur. To be preserved, the vein has to be dissected free from the arachnoid and cortex at a length of 10 to 20 mm.16 When an important vein ruptures, its reconstruction may be considered either by resuturing or by using the silicone tubing technique.17
Wounds made in a vein wall are common. Rather than coagulating the vein, hemostasis can be attempted by simply wrapping the wall with a small piece of Surgicel (Johnson and Johnson Medical, Viroflay, France). If this is insufficient, a very localized microcoagulation with a sharp bipolar forceps or by placing a single suture with a 10-0 nylon thread is recommended. In cases with a large defect, a patching repair can be performed.18,19 In all cases, whatever the technique used, hemostasis quality has to be checked by jugular compression at the neck.
Tumors invading the major dural sinuses
The study of long-term results in our series of 100 consecutive patients affected by meningiomas involving a major dural sinus, and in whom we attempted radical removal and venous repair,20 led us to the following conclusions. The low recurrence rate of 4% in our series, followed over a 3- to 23-year period (mean 8 years), supports resecting not only the tumor portion outside the sinus, but also the fragment invading the sinus. When radical removal is attempted, we consider venous reconstruction mandatory when the sinus is incompletely occluded, and potentially useful even in cases with complete occlusion. The goal is to restore the flow that might be compromised by impairment of the compensatory collateral channels (Figure 32–4). The traditional belief that radical removal of meningiomas with a totally occluded sinus is not dangerous must be reconsidered.21–24 In our series, the three patients who died (all three from brain swelling) had a meningioma that totally occluded the sinus and was wholly removed without any restoration of the sinus circulation.20
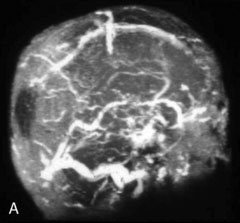
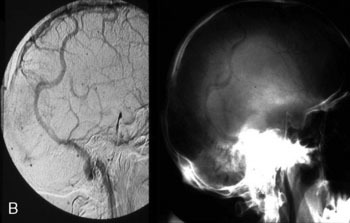
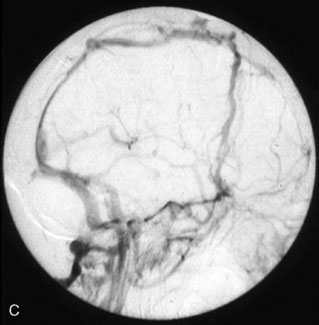
This is not surprising, as surgical access basically involves the destruction of some to all of the collateral pathways that naturally developed to compensate the sinus occlusion. Therefore, restoring the venous circulation at end of surgery may reduce brain swelling. Furthermore, patching or bypassing did not increase the morbidity rate in our series.20
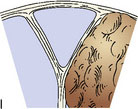
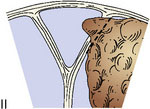
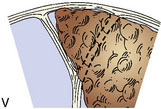
To guide in surgical decision making, we introduced a meningioma classification comprised of six types according to degree of sinus invasion1,22 (Figure 32–5). This simplified classification was developed after the ones introduced by Merrem,25 Krause,26 and Bonnal and Brotchi.27
< div class='tao-gold-member'>



Related posts:
 Using Cerebral Vaso-Reactivity in the Selection of Candidates for EC-IC Bypass Surgery
Using Cerebral Vaso-Reactivity in the Selection of Candidates for EC-IC Bypass Surgery
 Radial Artery Harvest for Cerebral Revascularization: Technical Pearls
Radial Artery Harvest for Cerebral Revascularization: Technical Pearls
 EC-IC Bypass Evidence
EC-IC Bypass Evidence
 Bypass Surgery for Complex MCA Aneurysms
Bypass Surgery for Complex MCA Aneurysms
 Endovascular Therapies for Cerebral Revascularization
Endovascular Therapies for Cerebral Revascularization
 EC-IC and IC-IC Bypass for Giant Aneurysms Using the ELANA Technique
EC-IC and IC-IC Bypass for Giant Aneurysms Using the ELANA Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


