CHAPTER 30 Intrasellar and Diaphragma Sellae Meningiomas 
INTRODUCTION
The first report of an intrasellar meningioma originating from the diaphragma sellae was published by Hardy and Robert in 1969;1 Cushing and Eisenhardt were the first to classify sellar and parasellar meningiomas.2 The suprasellar meningiomas as described by Cushing were further subdivided by Jefferson into diaphragma sella meningioma, tuberculum meningioma, and meningioma of the clinoid processes.3 Subsequently, Osama Al-Mefty proposed that diaphragma sellae meningioma had a clinical syndrome distinct from tuberculum sellae meningioma. He went on to classify the diaphragma sellae meningiomas into two supradiaphragmatic suprasellar types and one infradiaphragmatic intrasellar type.4 Diaphragma sellae meningiomas are rare, and intrasellar meningiomas originating from the dura of the sella turcica are even less commonly encountered.
REGIONAL ANATOMY
The surface area of the dura mater of the sella turcica is estimated to be greater than 6 cm2.5,6 Meningiomas can originate from the diaphragma sellae as well as any part of the dura mater of the sella turcica. Subdiaphragmatic intrasellar meningiomas are quite rare and only 18 operatively confirmed cases have been reported in the literature.6 The origins of 9 of the 18 reported cases of intrasellar meningiomas have been described. These include six meningiomas originating from the lower leaf of the diaphragma sellae, two from the floor of the sella turcica, and one from the anterior wall of the sella turcica.6 Meningiomas arising from the diaphragma sellae and the sellar dura must be distinguished from those arising from adjacent structures such as the planum sphenoidale, the tuberculum sellae, medial sphenoid wing, and cavernous sinus. In contrast to tuberculum sellae meningiomas that are most often fed by the posterior ethmoid arteries, diaphragma sellae meningiomas are supplied by branches of the internal carotid arteries. Intrasellar meningiomas are supplied by the dural branches of the external carotid artery, and branches of the internal maxillary artery as well as the internal carotid artery.6
CLASSIFICATION
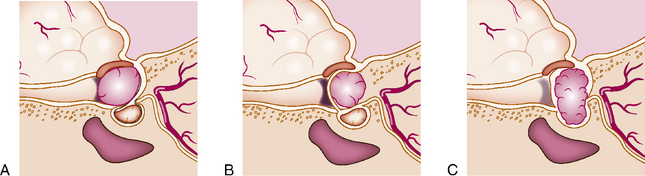
Al-Mefty and Ciric classified diaphragma sellae meningiomas into three types according to their site of origin4 (Fig. 30-1). Type A originates from the upper leaf of the diaphragma sellae anterior to the pituitary stalk. Type B arises from the upper leaf of the diaphragma sellae posterior to the pituitary stalk. Type C originates from the inferior leaf of the diaphragma sellae. Type A and B tumors are largely suprasellar, while type C diaphragma sellae meningiomas are largely intrasellar. Similar to type C, subdiaphragmatic meningiomas arising from the dura of the sella turcica are mostly intrasellar.
DIFFERENTIAL DIAGNOSIS
Pituitary adenoma; meningioma arising from adjacent structures such as the tuberculum, medial sphenoid wing, and cavernous sinus; craniopharyngioma; hemangiopericytoma; and metastasis should be considered in the differential diagnosis when evaluating patients with suspected diaphragma sellae or intrasellar meningiomas.7,8
CLINICAL FEATURES
Patients with diaphragma sellae and intrasellar meningiomas most commonly present with visual disturbance, visual field deficit, endocrine abnormalities, and headache. Al-Mefty and Ciric reported clinical symptoms and deficits in a series of 12 patients, 9 of whom had visual disturbance, 7 had visual field defects, 9 had headaches, and 2 had diabetes insipidus.4 The distinct clinical features of type A, B, and C diaphragma sellae meningiomas are presented in the text that follows.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


