Introduction
The objective of this chapter is to provide an introduction to the basic characteristics of magnetic resonance (MR) and computed axial tomographic (CAT) images. The physics of imaging is a fascinating and worthy subject, but it is not addressed here. The key things to be able to recognize first before looking for pathology are the imaging modality, plane and level of section, tissue characteristics, and whether a contrast agent has been administered. Sometimes this information is available by looking at the image annotations. Other times, for example, on certain board examination questions, this information must come from interpreting the image itself.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is a noninvasive method of imaging the central nervous system. It does not involve high-energy radiation. In essence, it is a technique for imaging brain water using gradient-localized radiofrequency waves. Contrast between tissues, for example, gray matter (GM) or white matter (WM), comes from small differences in the local magnetic environment of water in these tissues.
Magnetic Resonance Imaging Weighting
For the purposes of image interpretation, weighting refers to tissue contrast. At equilibrium, water in the central nervous system is magnetized in the same direction as the main magnetizing field, but only in the presence of this field. The strength of this main field gives the magnet its name, for example, 1.5 tesla, or 1.5 T units field strength. It takes high fields of this strength to produce an appreciable magnetization of water. Contrast depends on the recovery times (T1 and T2) of the magnetization of given tissue after radiofrequency pulses are applied. These pulses put the magnetized brain water out of equilibrium temporarily, producing a detectable signal. The T1 relaxation time is the time required for the bulk water to recover two thirds of its equilibrium T1 value, and T2 relaxation for it to lose two thirds of its signal value after a pulse. Because different tissue have different T1 and T2 relaxation times, these differences can be exploited to produce the different tissue contrasts in MRI.
T1-Weighted Images
These images are characterized by a relatively hyperintense signal of the WM in relation to the GM. Cerebrospinal fluid (CSF) is relatively hypointense on T1-weighted images, below the signal intensity of GM. Scalp and muscle tissue appears gray (single arrowhead), but subcutaneous scalp (double arrowheads) and other fat-containing tissues are relatively hyperintense. The single line indicates fatty marrow within the diploe of the skull; the inner and outer bony tables of the skull are hypointense, as is other bone (see Figure I.1).
Inversion Recovery
These are heavily T1-weighted images that provide excellent anatomic detail because of the strong contrast between WM and GM. They are particularly helpful in pediatric studies performed to demonstrate cortical migrational defects or other developmental brain anomalies (see Figure I.2).
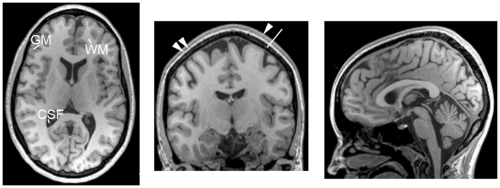 Figure I.1 Left—axial slice at level of the thalamus; middle—coronal at level of the thalamus and hippocampus; right—midline sagittal section showing corpus callosum, pituitary, cerebellar vermis, and other normal midline structures. GM, gray matter; WM, white matter; CSF, cerebrospinal fluid |
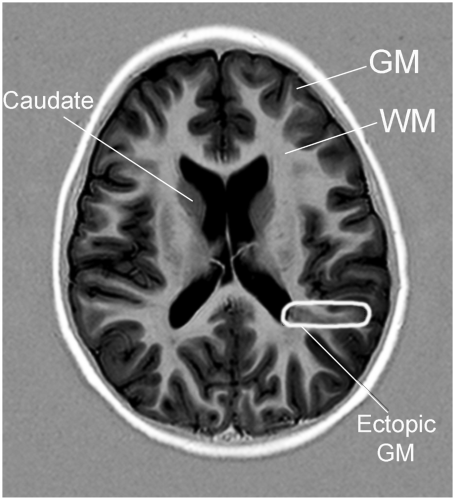 Figure I.2 The axial inversion recovery (IR) image demonstrates focal cortical dysplasia in the left temporal region (drawn oval). GM, gray matter; WM, white matter |
T2-Weighted Images
This weighting is characterized by a relatively hypointense signal of the white matter in relation to the grey matter. The CSF on T2-weighted images is above the signal intensity of grey matter. Scalp, adipose, and subcutaneous tissue appears bright (single arrowhead). See Figure I.3.
Fluid Attenuated Inversion Recovery (FLAIR)
Fluid attenuated inversion recovery (FLAIR) is a T2-weighted sequence that suppresses the signal from CSF and produces a heavy T2 weighting. As in other T2-weighted sequences, it is characterized by a relatively hypointense signal of WM in relation to GM (note the relatively low signal in the anterior commissure [AC], a myelinated interhemispheric tract). Suppression of CSF gives FLAIR a particular advantage in distinguishing lesions in the periventricular and sulcal regions. See Figure I.4 and Table I.1.1
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


