The outermost layer of Figure 8.1 comprises informal influences on problem drinkers: the work colleague who advises that a career may be damaged if drinking is not stopped, the husband who supports his wife as she tries to get away from the bottle, the friends who praise or mock a newly abstinent chum’s lifestyle, the Internet questionnaire that asks “Do you have a drinking problem?” These influences were addressed primarily in Section 1, although their role is felt in Section 2 because informal influence can spur or deter help-seeking from formal sources of help, as shown in Figure 8.1’s inner two circles.
The middle area of Figure 8.1 is the nonspecialist sector, those agencies that may offer support or apply pressure (or both) to problem drinkers even though their raison d’être is not related to alcohol. The hidden majority of problem drinkers daily rub shoulders with fellow members of their community in these settings; for example, when they consult their primary care doctors or have the misfortune to attend the Emergency Room. Therefore, any approach to the treatment of drinking problems must consider the many different settings in which these develop and present. These settings are described in detail in Chapter 9.
Finally, the innermost circle of Figure 8.1 is the specialist sector, namely professional services (see Chapter 13) and mutual-help programmes (see Chapter 14) with the explicit purpose of helping problem drinkers. Their location at the centre of the diagram is not specialist narcissism. Rather, it reflects specialist treatment being where a small minority of all drinking problems is handled and, indeed, that the other influences in the larger circles of the chart are often sufficient to bring a drinking problem to heel.
Trajectories of help-seeking and progress or regress in the drinking problem
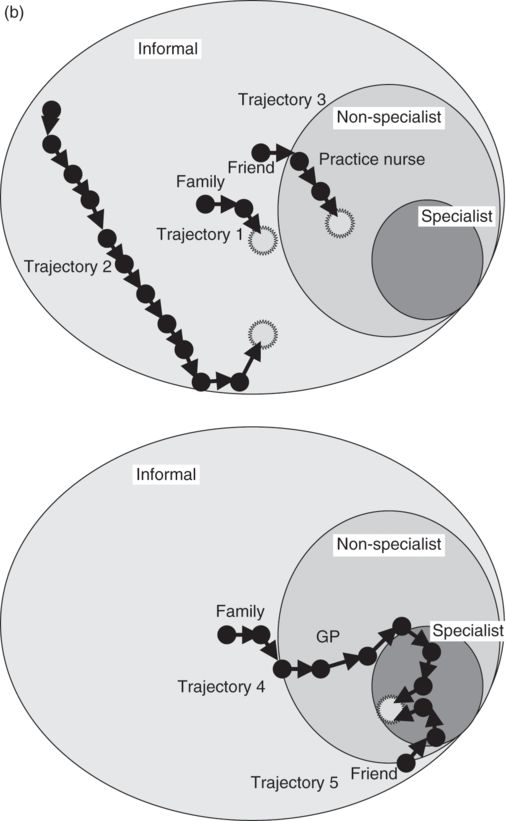
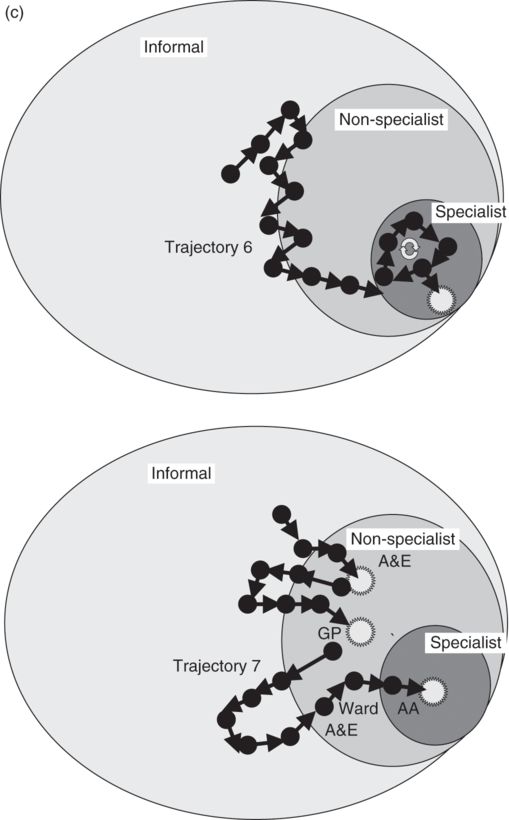
The help-seeking pathway of most individuals will not be straightforward but in fact rather “messy” because they will derive varying degrees of parallel support from informal, nonspecialist, and specialist sources that vary over the time course. Although multiple sources of treatment can be accessed simultaneously, the position of the treatment arrow on Figure 8.1 highlights the treatment source that is “making the running” at any one particular time. The temporary or sustained treatment goal is depicted by the star, and many treatment paths may not terminate in one. Furthermore, there are multiple permutations of these treatment trajectories that occur in various combinations, with associated gaps, pauses, and delays. Whilst the treatment arrows build into a trajectory that is unique for that individual, characteristic patterns may also be recognized.
Many will manage their drinking problem without accessing specialist or nonspecialist services, using the informal support of family and friends to achieve their goal, either rapidly as shown by trajectory 1 in Figure 8.1b or over a longer period as depicted in trajectory 2. Others will approach nonspecialist services, such as their practice nurse, who may assist by using a brief intervention (trajectory 3). An example of the stepped-care model is presented in trajectory 4, in which specialist alcohol treatment is reserved for those who do not respond to simpler approaches (Bower & Gilbody, 2005). In this example, concerned relatives advise the individual to cut down, and, when this fails for the second time, the individual consults their general practitioner who provides community detoxification. Several weeks later, the patient relapses, continuing drinking during a second attempted community detoxification. The general practitioner then refers them to the specialist services, and, following detailed assessment, in-patient detoxification is arranged followed by residential rehabilitation. The individual then successfully maintains a prolonged period of abstinence with the support of Alcoholics Anonymous.
Some see stepped care as providing specialist input to those who have “failed” at other approaches, thereby delaying access to the needed treatment. Therefore, an important aspect of stepped care is a mechanism for self-correction that monitors progress and provides for the “stepping up” of treatment as required. In addition, accurate assessment in the early stages of presentation is vital because this can identify an individual who needs direct access to specialist care and thereby prevent the delay and negative impact associated with multiple failures at lower intensity interventions. Indeed, in trajectory 5 in Figure 8.1b, a friend at work who has experienced a drinking problem advised the individual to attend the open-access assessment clinic with the local community alcohol team; the team recommends a course of individual counselling. An early accurate assessment enabled this individual to be identified and referred to a supportive resource.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


