♦ Preoperative
Patient Preparation
- Clear liquid diet the day prior to surgery
- Bowel prep with magnesium citrate and fleet enema the night prior to surgery
Operative Planning
- Review imaging (roentgenograms, magnetic resonance imaging) to study the spine and vascular anatomy
Equipment
- Radiolucent operating room table
- Laparoscopic set-up (camera, monitor, ports, CO2)
- Laparoscopic vascular clips
- Anterior lumbar interbody fusion tray
Operating Room Set-up
- Bipolar cautery
- Fluoroscope
♦ Intraoperative
Positioning
- Supine with left arm over patient’s chest or in the cruciate position
- Patient should be placed in ~30 degrees of Trendelenburg with care to secure the patient to the table.
- Ensure adequate visualization with the fluoroscope.
- Drape the abdomen to include the area overlying the iliac crest and the suprapubic region.
Sterile Scrub and Preparation
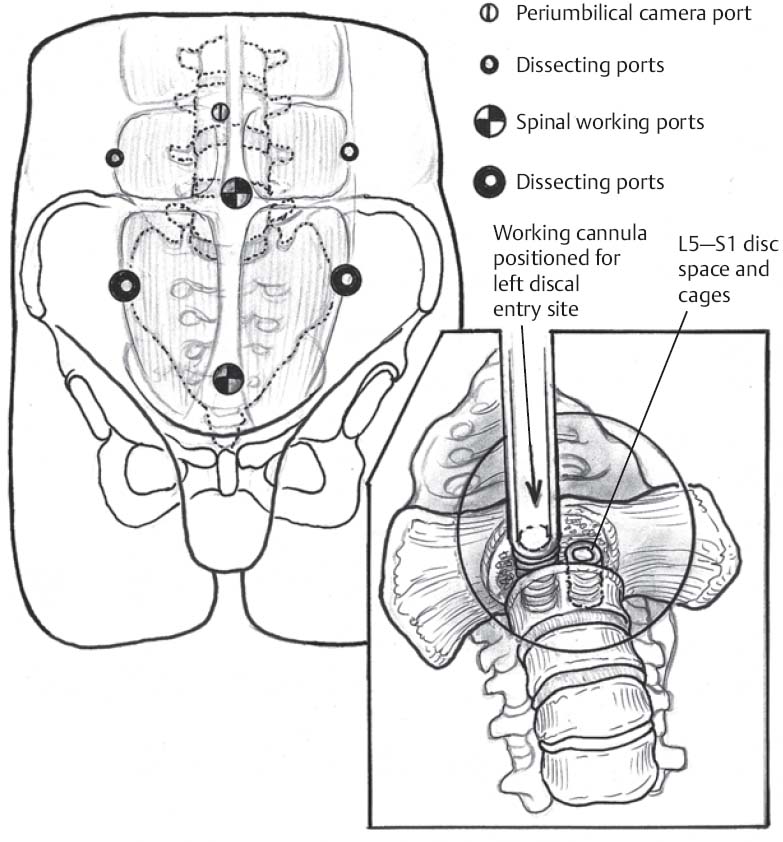
Port Placement (Fig. 117.1)
- The first portal placed is the periumbilical portal (12 mm port). Insert using the open (Hasson) technique via a semicircular incision about the inferior edge of the umbilicus.
- Insufflate the peritoneal cavity with CO2 prior to placement of additional portals.
- Place two lateral 5 mm ports: equidistant from the pubis and umbilicus and lateral to the rectus muscle.
- An optional portal may be placed at the level of the umbilicus, lateral to the left lateral portal. This may be used for retraction of the sigmoid mesocolon, if needed.
- The suprapubic portal is placed after direct visualization of the disc space.
L5–S1 Exposure
- Make a 3 cm vertical incision in the posterior peritoneum, right of the midline of the spine.
- Identify a loose areolar plane anterior to the spine. Within this plane is the parasympathetic plexus. Bluntly sweep laterally with a Kittner.
- Small vessel bleeding should be controlled with bipolar cautery. Avoid the use of monopolar cautery as it may damage the parasympathetic plexus and lead to retrograde ejaculation.
- Identify the middle sacral artery and vein. Dissect free from adjacent structures and ligate with vascular clips.
- Visualize the iliac vessels on either side of the disc space.
- Confirm the level via fluoroscopy.
L4–L5 Exposure
- Exposure of this level may be more difficult via this approach because of the patient’s vascular anatomy. Three scenarios may be present: a high bifurcation about the L4–L5 disc space, a low bifurcation below the L4–L5 disc space, and the most common, a bifurcation at the level of the disc space.
- In the scenario of a high bifurcation, expose the disc space between the vessels as in a L5–S1 disc.
- In the scenario of a low bifurcation, approach the L4–L5 disk to the left of the aorta and vena cava, retracting these structures to the right.
- Prior to retracting the vena cava, identify and ligate the left iliolumbar vein vessels.
- In the scenario of bifurcation at the level of the disc space, the ideal approach must be determined intraoperatively.
Only gold members can continue reading. Log In or Register to continue







