(1)
Marina Spine Center, Marina del Rey, CA, USA
The lateral approach to the cervical spine, when combined with the more proximal detachment of the sternocleidomastoid muscle, as in the anterolateral C1–C3 approach, and with the more distal partial detachment of sternocleidomastoid muscle from the clavicle, as in the Nanson supraclavicular approach, allows good exposure from C1 to T2. The standard midcervical approach to the lateral spine C3–C7 as described by Hodgson is lateral to the sternocleidomastoid muscle and lateral to the carotid sheath. The approach is in a relatively avascular plane avoiding the medial neurovascular structures but is more restrictive in its exposure.
Get Clinical Tree app for offline access

1.
Position the patient with the head turned to the left. Make a transverse incision in a skin crease at an appropriate level in the neck to correspond with the level of the spine. The approach is from the right side and extends from the posterior border of sternocleidomastoid approximately 4 inches toward the midline [1] (Fig. 9.1).
Fig. 9.1
The lateral approach to the cervical spine can be used for C3–C7. The transverse incision is made at the appropriate level, and dissection is carried through the skin and platysma muscle as in any of the standard approaches to this area
2.
Divide subcutaneous tissue and platysma muscle. Ligate any large branches of the external jugular vein present in the wound and retract cutaneous nerves when possible.
3.
Identify the medial and lateral borders of the sternocleidomastoid muscle and retract its lateral border medially (Fig. 9.2). If there is an impediment to retraction, the sternocleidomastoid can be wholly or partially divided.
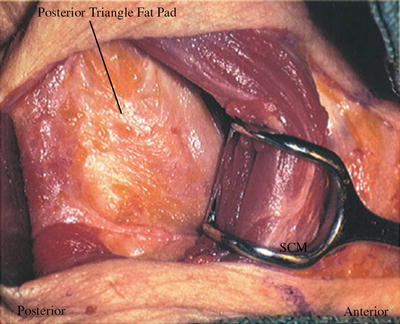
Fig. 9.2
Identify the medial and lateral borders of the sternocleidomastoid muscle and retract its lateral border medially. If there is an impediment to retraction, the sternocleidomastoid can be wholly or partially divided. Identify the fat pad of the posterior triangle
4.
Identify the fat pad of the posterior triangle [1] (Fig. 9.3). Blunt dissection and finger palpation should follow the fat pad through the posterior triangle to the spine.