Limbs
reflexes and sensation
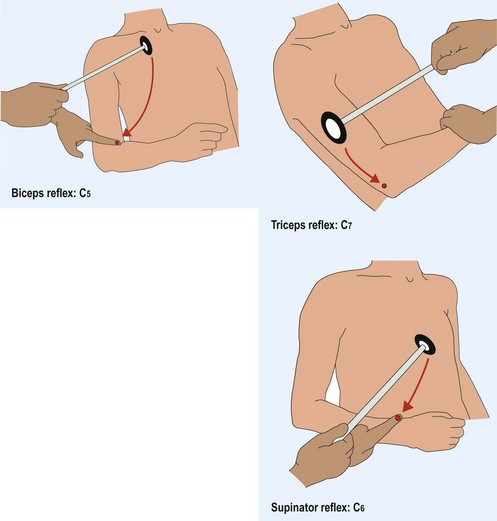
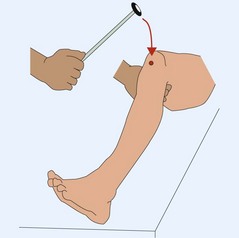
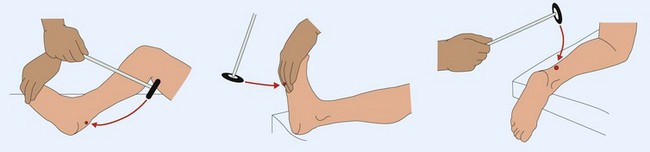
How to elicit tendon reflexes
The patient needs to be relaxed, with the muscle to be tested in the middle of its range of movement (Figs 1–3). The tendon hammer is swung to hit the tendon or, for the biceps and supinator reflexes, a finger on the tendon. The muscle is watched for movement in response to this. If the reflex is not obtainable then the patient is asked either to clench the teeth or make a fist – reinforcement – which may allow the reflex to be found. When testing the reflexes it is useful to remind yourself of the segmental level being tested.