SECTION IV LOCALISED NEUROLOGICAL DISEASE AND ITS MANAGEMENT B. SPINAL CORD AND ROOTS
SPINAL CORD AND ROOTS
Disorders localised to the spinal cord or nerve roots are detailed below, but note that many diffuse neurological disease processes also affect the cord (see Section V, e.g. multiple sclerosis, Friedreich’s ataxia).
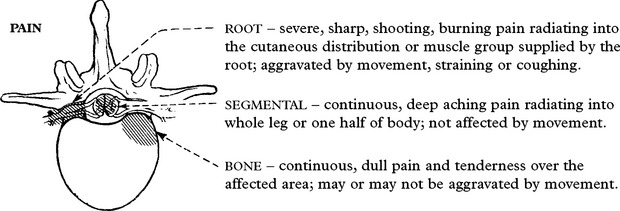
SPINAL CORD AND ROOT COMPRESSION – NEUROLOGICAL EFFECTS
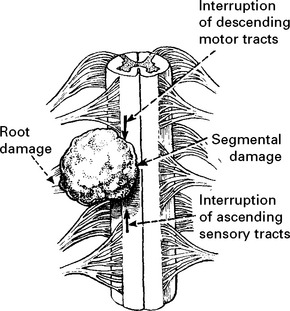
LATERAL COMPRESSIVE LESION
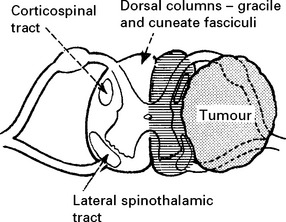
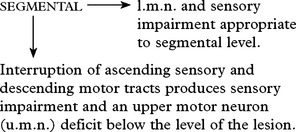
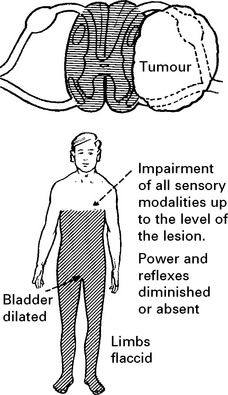
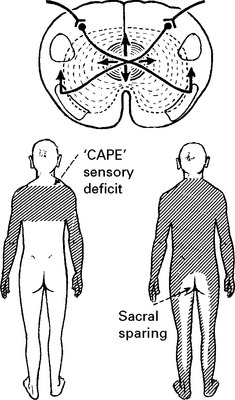
Long tract – signs and symptoms Partial (Unilateral) cord lesion
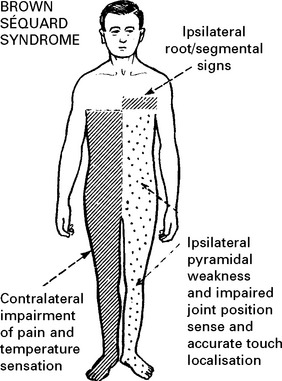
UPPER MOTOR NEURON (u.m.n.) signs (maximal on side of lesion):
Damage to sympathetic pathways in the T1 root or cervical cord causes an ipsilateral Horner’s syndrome (page 145).
SPINAL CORD AND ROOT COMPRESSION – INVESTIGATIONS
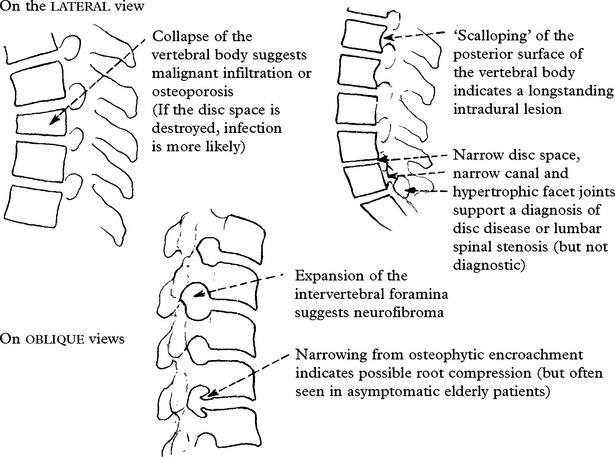
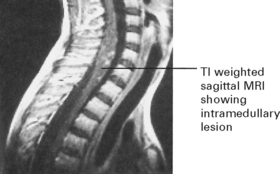
MRI

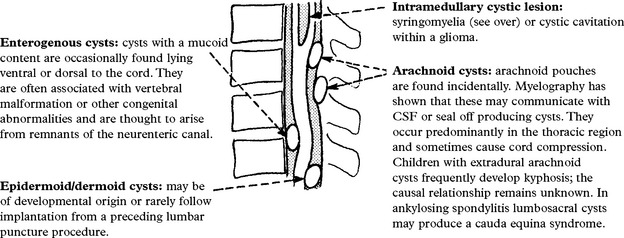
MRI differentiates a syrinx (page 401) or a cystic swelling within the spinal cord from a solid intramedullary tumour (page 400).
MYELOGRAPHY
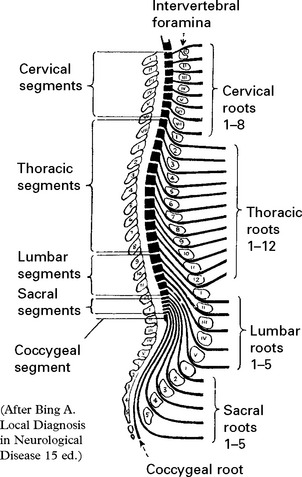
Lesions in the lumbar and sacral regions require a ‘radiculogram’, outlining the lumbosacral roots.
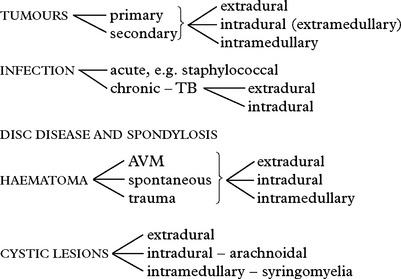
SPINAL CORD AND ROOT COMPRESSION
TUMOURS
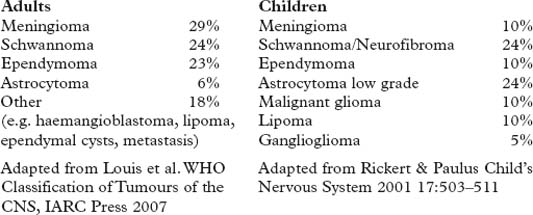
Pathology: The pathological features of spinal tumours match those of their intracranial counterparts (see page 303).
METASTATIC TUMOUR
Occurs in 5% of all cancer patients and accounts for 50% of adult acute myelopathies.
Primary site: Usually breast, lung, prostate, kidney or myeloma (see below).
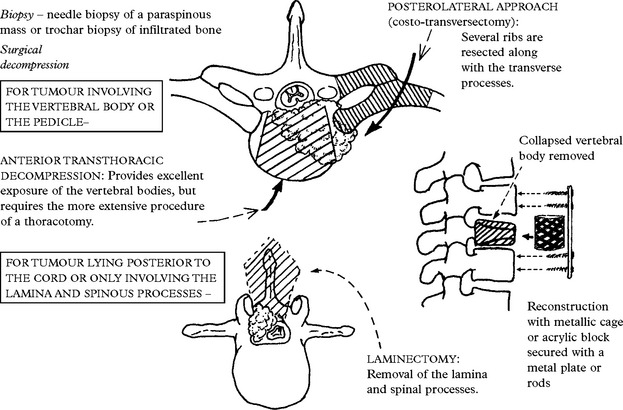
MANAGEMENT SCHEME
All patients require steroids and biopsy if no prior diagnosis exists.
| Decompressive surgery (plus radiotherapy) | Radiotherapy |
|---|---|
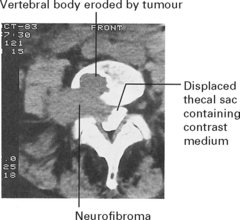
SCHWANNOMA/NEUROFIBROMA
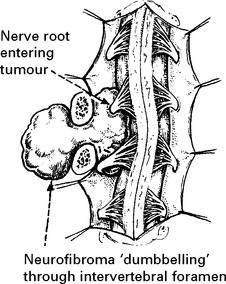
Neurofibromas are identical apart from their microscopic appearance (page 304) and their association with multiple neurofibromatosis (Von Recklinghausen’s disease NF1 – see page 561) – look for café au lait patches in the skin.
MRI or CT myelography identifies an intradural/extramedullary lesion. Axial views will delineate any extraspinal extension (see page 395). Complete operative removal is feasible but the nerve root of origin is inevitably sacrificed. Overlap from adjacent nerve roots usually minimises any resultant neurological deficit.
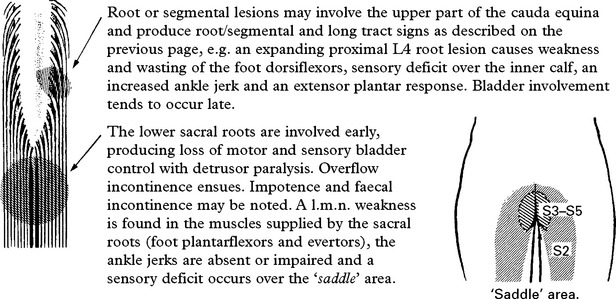
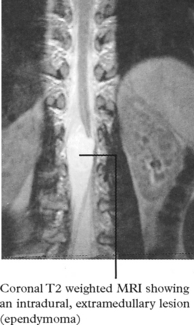
EPENDYMOMA OF THE CAUDA EQUINA
Over 50% of spinal ependymomas occur around the cauda equina and present with a central cauda equina syndrome (page 394). Operative removal combined with radiotherapy usually gives good long-term results, although metastatic seeding occasionally occurs through the CSF.
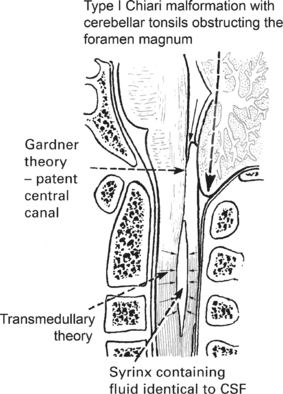
SYRINGOMYELIA
Syringomyelia is the acquired development of a cavity (syrinx) within the central spinal cord. The lower cervical segments are usually affected, but extension may occur upwards into the brain stem (syringobulbia, see page 381) or downwards as far as the filum terminale.
The cavitation appears to develop in association with obstruction:
Pathogenesis
< div class='tao-gold-member'>
Related posts:
 CLINICAL PRESENTATION, ANATOMICAL CONCEPTS AND DIAGNOSTIC APPROACH
CLINICAL PRESENTATION, ANATOMICAL CONCEPTS AND DIAGNOSTIC APPROACH
 LOCALISED NEUROLOGICAL DISEASE AND ITS MANAGEMENT C. PERIPHERAL NERVE AND MUSCLE
LOCALISED NEUROLOGICAL DISEASE AND ITS MANAGEMENT C. PERIPHERAL NERVE AND MUSCLE
 GENERAL APPROACH TO HISTORY AND EXAMINATION
GENERAL APPROACH TO HISTORY AND EXAMINATION
 INVESTIGATIONS OF THE CENTRAL AND PERIPHERAL NERVOUS SYSTEMS
INVESTIGATIONS OF THE CENTRAL AND PERIPHERAL NERVOUS SYSTEMS
 LOCALISED NEUROLOGICAL DISEASE AND ITS MANAGEMENT A. INTRACRANIAL
LOCALISED NEUROLOGICAL DISEASE AND ITS MANAGEMENT A. INTRACRANIAL
 MULTIFOCAL NEUROLOGICAL DISEASE AND ITS MANAGEMENT
MULTIFOCAL NEUROLOGICAL DISEASE AND ITS MANAGEMENT
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


