Macrocephaly
Susan I. Blaser, MD, FRCPC
DIFFERENTIAL DIAGNOSIS
Common
Benign Familial Macrocrania
Hydrocephalus and Obstructed CSF Spaces
Intraventricular Hemorrhage
Aqueductal Stenosis
Arachnoid Cyst
Enlarged Subarachnoid Spaces
Villous Hypertrophy of the Choroid Plexus
Subdural Hematoma, Chronic
Less Common
Dandy-Walker Continuum
Neoplasm
Glioblastoma Multiforme
Teratoma
Neurocutaneous Disorders
Neurofibromatosis Type 1
Tuberous Sclerosis Complex
Hemimegalencephaly
Megalencephaly Syndromes
Rare but Important
Hydranencephaly
Inborn Errors of Metabolism
Glutaric Aciduria Type 1
MLC1
Mucopolysaccharidosis
Alexander Disease
Canavan Disease
Achondroplasia
Fibrous Dysplasia
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Macrocephaly = head circumference > 2 standard deviations above mean for age-matched controls
Macrocephaly = macrocrania
Megalencephaly = subtype of macrocrania
Imaging infants/children with macrocephaly
Hydrocephalus or white matter abnormality found? Use contrast!
Glutaric aciduria type 1 = child abuse mimic
Helpful Clues for Common Diagnoses
Benign Familial Macrocrania
Family history important
Intraventricular Hemorrhage
Hemosiderin not always apparent on follow-up images
Aqueductal Stenosis
Look for associated hemosiderin, vascular anomalies
Arachnoid Cyst
Steady-state acquisition sequence to identify cyst wall
Enlarged Subarachnoid Spaces
Look for traversing veins
Natural history: Resolution by 12-18 months
Villous Hypertrophy of the Choroid Plexus
Likely on a spectrum, including choroid plexus papilloma
Bilateral choroid plexus lesions typical
Subdural Hematoma, Chronic
MR identifies hemorrhagic components
Helpful Clues for Less Common Diagnoses
Dandy-Walker Continuum
Classic Dandy-Walker & Blake pouch cyst: Vermian angulation, large bony posterior fossa
Classic Dandy-Walker
Incompletely lobulated vermis, deficient fastigial recess/primary fissure
Blake pouch cyst
Intact vermis, fastigial recess, and primary fissure
Neoplasm
Large, bulky neonatal tumors
Glioblastoma Multiforme
Enhancement, necrosis, hemorrhage
Teratoma
Fat, calcium, enhancing soft tissue
Neurofibromatosis Type 1
Look for foci of abnormal signal intensity (FASI), optic nerve gliomas, café-au-lait spots
Macrocrania predominantly derived from bulky white matter
Tuberous Sclerosis Complex
Cutaneous markers (ash-leaf spots) may be occult in 1st year of life
Look for Ca++ subependymal nodules, radial lines
Hemimegalencephaly
Look for cutaneous markers & stigmata of overgrowth syndromes
Hypomelanosis of Ito
Proteus syndrome
Linear sebaceous nevus syndrome
Megalencephaly Syndromes
Clues in name
Megalencephaly, polymicrogyria syndrome
Megalencephaly with dilated Virchow-Robin spaces
Cerebral gigantism (Soto syndrome)
Macrocrania-cutis marmorata telangiectatica congenita
Helpful Clues for Rare Diagnoses
Hydranencephaly
Distinguish from maximal hydrocephalus
MR shows cortex, falx
Glutaric Aciduria Type 1
Bilateral temporal lobe hypoplasia & large sylvian fissures
Resembles bilateral middle cranial fossa arachnoid cysts
Crisis: Caudate, putamen, globus pallidus swelling, & ↑ signal
MLC1
Diffusely ↑ white matter signal
Temporal pole & frontoparietal cysts
Macrocrania differentiates from CMV (common microcephaly)
Mucopolysaccharidosis
Dilated perivascular spaces
Alexander Disease
Enhancement is the key to diagnosis!
Infant: Frontal swelling & ↑ signal & enhancement
Juvenile: Brainstem foci of ↑ signal & enhancement
Canavan Disease
MRS key: ↑ ↑ NAA
Achondroplasia
Small skull base
Jugular foramina coarctation: CSF drainage impaired
Foramen magnum coarctation: Cervicomedullary compression
Fibrous Dysplasia
Focal or diffuse (leontiasis ossea) may ↑ head circumference
Classic radiograph/CT: Ground-glass
MR (T2): Black velvet appearance
SELECTED REFERENCES
1. Colombani M et al: A new case of megalencephaly and perisylvian polymicrogyria with post-axial polydactyly and hydrocephalus: MPPH syndrome. Eur J Med Genet. 49(6):466-71, 2006
2. Groeschel S et al: Magnetic resonance imaging and proton magnetic resonance spectroscopy of megalencephaly and dilated Virchow-Robin spaces. Pediatr Neurol. 34(1):35-40, 2006
3. D’Ambrosio AL et al: Villous hypertrophy versus choroid plexus papilloma: a case report demonstrating a diagnostic role for the proliferation index. Pediatr Neurosurg. 39(2):91-6, 2003
4. Medina LS et al: Children with macrocrania: clinical and imaging predictors of disorders requiring surgery. AJNR Am J Neuroradiol. 22(3):564-70, 2001
5. Wilms G et al: CT and MR in infants with pericerebral collections and macrocephaly: benign enlargement of the subarachnoid spaces versus subdural collections. AJNR Am J Neuroradiol. 14(4):855-60, 1993
Image Gallery
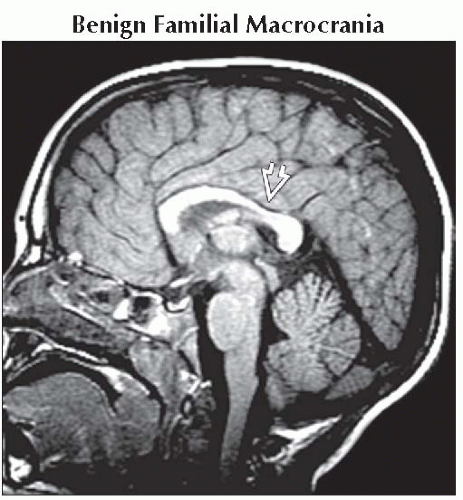 Sagittal T1WI MR shows a normal-appearing corpus callosum and callosal isthmus  , gyral pattern, myelin maturation, and midline structures in this child with benign familial macrocrania. , gyral pattern, myelin maturation, and midline structures in this child with benign familial macrocrania. |
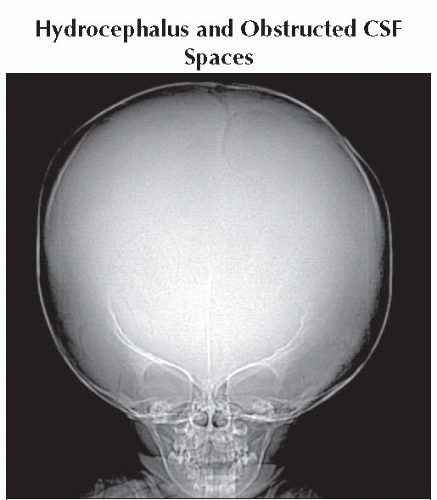 Anteroposterior radiograph shows massive macrocrania in a child with untreated hydrocephalus. |
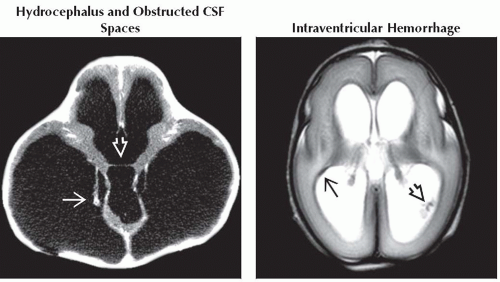 (Left) Axial NECT shows massive tri-ventricular hydrocephalus. The choroid plexus dangles in the fluid  , and the massa intermedia , and the massa intermedia  is stretched thin. (Right) Axial T2WI MR in a 27 week gestational age (corrected) premature infant shows an age-appropriate immature sulcal pattern. There is a small focus of ependymal hemosiderin is stretched thin. (Right) Axial T2WI MR in a 27 week gestational age (corrected) premature infant shows an age-appropriate immature sulcal pattern. There is a small focus of ependymal hemosiderin  in the right trigone, a small clot in the right trigone, a small clot  in the left. in the left. |
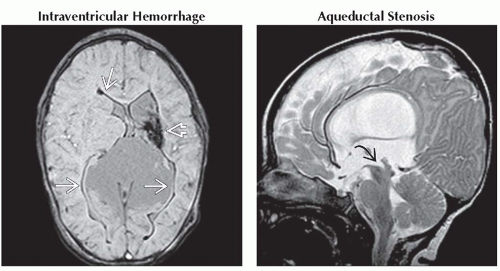 (Left) Axial T2* GRE MR in an infant born prematurely with shunted hydrocephalus shows evidence of hemosiderin and volume loss in left caudothalamic groove
 . Diffuse hemosiderin staining . Diffuse hemosiderin staining  of the ependyma follows remote IVH. (Right) Sagittal T2WI MR shows hydrocephalus and a funnel-shaped aqueduct of Sylvius of the ependyma follows remote IVH. (Right) Sagittal T2WI MR shows hydrocephalus and a funnel-shaped aqueduct of Sylvius  . The appearance is typical, with the proximal aqueduct splayed and the distal aqueduct closed. . The appearance is typical, with the proximal aqueduct splayed and the distal aqueduct closed.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|