Chapter 40 Management of Wound Dehiscence in Spinal Tumor Surgery
INTRODUCTION
The development of wound dehiscence and infection after spinal surgery for tumors is sometimes encountered. The incidence of superficial or deep wound infections is very high in patients who received preoperative radiation. The rate of infection in this patient group is about 10%. Patients requiring operation within a 6-week period after irradiation are at extremely high risk for developing wound complications.1 Acute radiation effects include inhibition of fibroblast outgrowth, resulting in a reduction of collagen formation and tensile wound strength. Many surgeons emphasize the importance of avoiding preoperative radiotherapy in patients who are candidates for surgery as a first-line therapy.2 The other risk factors for wound-related complications include the use of instrumentation, medical comorbidities, malnourishment, negative protein balance, multiple prior operations, and high-dose corticosteroid agents.1 In many patients, little can be done to ameliorate these risk factors; however, timely intervention may decrease the risk of other morbidities such as septicemia and deep venous thrombosis. In the past, wound correction has required serial debridements and raised significant concerns regarding instrumentation salvage.3 Recently, several authors have shown that instrumentation salvage is possible when using techniques such as serial debridements with antibiotic-impregnated beads, irrigation-suction systems, or muscle flaps.4 The trapezius or latissimus dorsi muscle turnover flaps and paraspinous advancement flaps are commonly used to treat wound dehiscence in patients undergoing surgery for spinal tumors. Flap selection for spinal wound repair is based on the anatomical location of the defect. The flap of choice for cervical spinal wound is the trapezius as a muscle only or as a musculocutaneous flap, based on the transverse cervical artery. For reconstruction of lower thoracic or upper lumbar spinal wounds, the latissimus dorsi muscle flap is the first choice. For the lower lumbar level wound, the paraspinal muscle flap is chosen. These muscle flaps provide vascularized muscle coverage that allows for instrumentation salvage with a limited number of wound debridements.
SURGICAL TECHNIQUES
TRAPEZIUS TRANSPOSITIONAL FLAP
The trapezius muscle originates from the occipital bone and the seventh cervical and all thoracic vertebrae and inserts into the spine of the scapula, acromion, and clavicle. The muscle suspends the shoulder girdle and assists in raising and rotating the shoulder. The accessory nerve provides the innervation. The main blood supply to the trapezius muscle and overlying skin is from superficial and deep descending branches of the transverse cervical artery. The transverse cervical artery enters the trapezius muscle at the base of the neck and descends vertically along the deep surface of the trapezius muscle. The superficial descending branch often arises directly from the thyrocervical trunk and is named the transverse cervical artery. In this event, the deep descending branch arises directly from the subclavian artery and is termed the dorsal scapular artery. Generally, this area is not dissected during routine vertical trapezius flap harvesting. The dorsal scapular artery runs under the levator muscle, and its major branch penetrates between the rhomboid muscles and descends along the deep surface of the trapezius to supply the lower third of the trapezius.5 As a result, the muscle and overlying skin below the tip of the scapula generally receive their dominant blood supply from the dorsal scapular artery. The muscle and overlying skin above the tip of the scapula generally receive their dominant blood supply from the transverse cervical artery.6
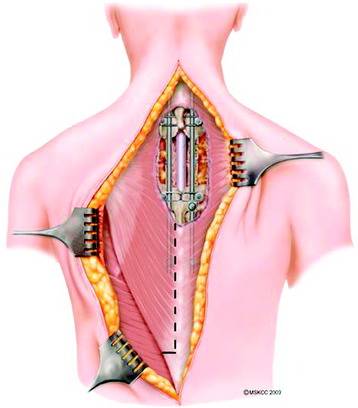
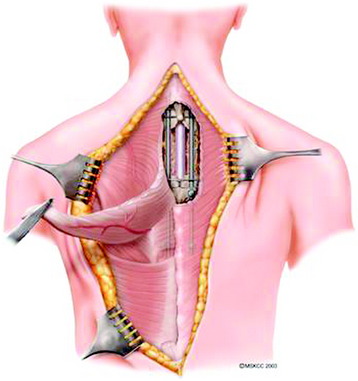
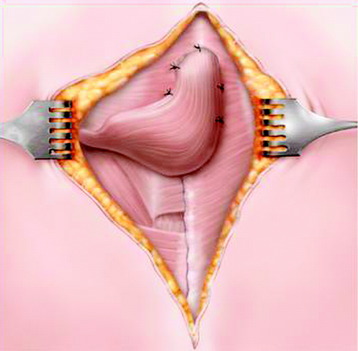
Trapezius muscle transpositional flaps are harvested through a midline incision in the region of the muscle, typically extending from the existing cervicothoracic incision inferiorly to the tip of the muscle. Skin and subcutaneous tissues are elevated, exposing the inferior half of the muscle, and the tissues are detached and elevated to the level of the scapula (Figs. 40-1 and 40-2). Care is taken to preserve the descending branch of the transverse cervical artery. The flap is turned on itself and transposed to obliterate the dead space and to cover the hardware of the cervical or upper thoracic defect (Fig. 40-3). As with all flaps, closed suction drains are placed under the skin flaps, and a layered skin closure is performed.
LATISSIMUS DORSI TRANSPOSITIONAL FLAP
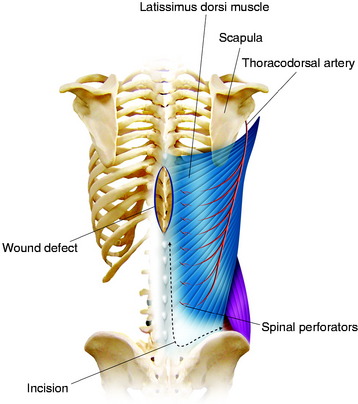
The transposition technique is first described (Figs. 40-4 and 40-5).7 After an appropriate size is outlined, the distal portion of the flap is incised. The incision is carried down through the thoracolumbar fascia. The dissection moves in this subfascial plane and in a cephalic direction until sufficient tissue is mobilized to meet the requirements of the defect. The lower attachment of the latissimus dorsi is incised; however, the spinal attachment to the muscle is preserved as much as possible. The humeral attachment is never released. Care should be taken to preserve as many posterior perforators of the lumbar and lower intercostal arteries as possible while still transferring a quantity of tissue that conforms well to the wound bed. To achieve wound closure in more caudal wounds, an island gluteus maximus flap based on its superior gluteal vascular pedicle can be transposed. A latissimus dorsi fasciocutaneous flap can cover fairly large defects if the wound is located mostly in the lower thoracic and upper to mid-lumbar area. In the lower thoracic and lumbar areas of the back, the local options for muscle flap reconstruction are anatomically limited. Essentially, three muscles lie nearby: the erector spinae muscle group, the latissimus dorsi muscle, and the gluteus maximus muscle.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


