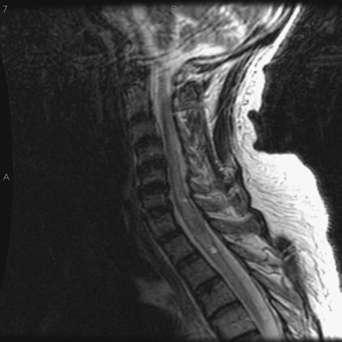
67 A 66-year-old man with non–small-cell lung cancer developed lower extremity weakness and incontinence over a period of days. He was paraparetic on examination, but did not have spine tenderness to percussion. A complete spine magnetic resonance imaging (MRI) did not show any cord compression. Cervical MRI (Fig. 67-1) shows enlargement of the spinal cord by an intramedullary lesion. Intramedullary metastatic spine lesion Spinal radiation was given. Although the most common intramedullary spinal cord lesions are astrocytoma, ependymoma, and hemangioblastoma, intramedullary metastases are on the rare end of the spectrum. Less than 1% of all spinal cord tumors can be categorized as such. Lung and breast are the most common primaries, but renal and gastrointestinal carcinomas have also contributed to the case report literature on cord metastases. One may also see drop metastases from primary brain lesions. Hemicord symptoms are not uncommonly described. Both surgery and radiation have been described with varied results.
Metastatic Spinal Cord Lesion
Presentation
Radiologic Findings
Diagnosis
Treatment
Discussion
Metastatic Spinal Cord Lesion
Only gold members can continue reading. Log In or Register to continue







Full access? Get Clinical Tree


