15 Minimally Invasive EC-IC Bypass Procedures and Introduction of the IMA-MCA Bypass Procedure
Minimally invasive superficial temporal artery to middle cerebral artery bypass through a bur hole
STA-MCA bypasses are established EC-IC bypasses for low to moderate flow cerebral revascularization. A STA-MCA, low-flow, EC-IC bypass traditionally requires a large frontotemporal craniotomy to expose the distal Sylvian fissure for the anastomotic site. We describe a less-invasive procedure using a single 2- to 2.5-cm enlarged bur hole, in place of the standard craniotomy, through which the recipient and donor vessels were identified and the anastomosis performed.1
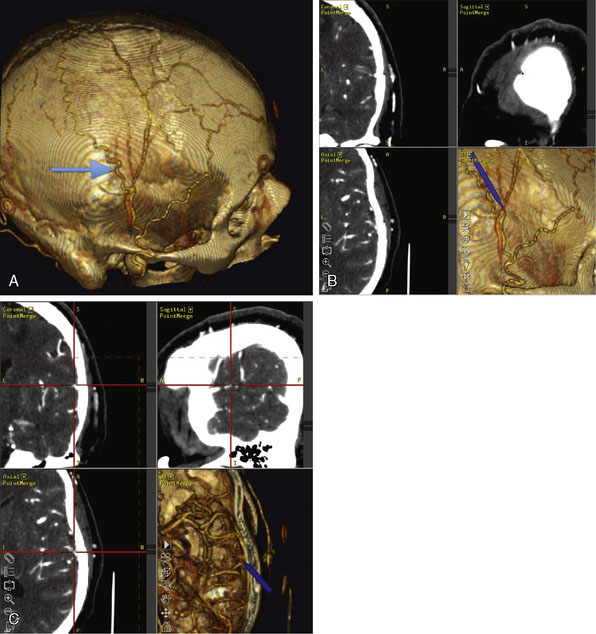
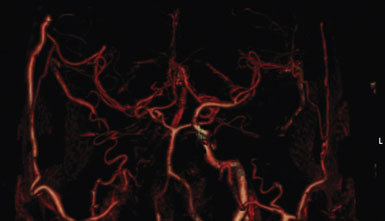
This procedure was performed for multiple patients with recurrent cerebrovascular ischemic episodes. One patient was awake for the procedure, with local anesthesia and propofol sedation, due to his multivessel occlusive disease and compromised vascular reserve, in an effort to avoid general anesthesia-related hypotension. With the aid of a stereotactic neuronavigation system, we minimized the size of the skin incision and the craniotomy such that the procedure could be performed effectively via an enlarged bur hole or small craniotomy (2- to 2.5-cm diameter). A CT angiogram was used preoperatively to select the donor vessel, recipient vessel, and anastomosis site. The STA was visualized, along with its frontal and parietal branches. The diameters of the branches were measured in order to identify the optimal donor vessel (Figure 15–1A). A linear skin incision was then made overlying the donor vessel. Bur hole/craniotomy placement can be planned preoperatively using a stereotactically reconstructed model based on the CT angiogram (Figure 15–1B). The recipient vessel is chosen according to its caliber and superficial location in the Sylvian fissure. The optimal recipient vessel is identified on review of the CT angiogram (Figure 15–1C). The exact location of the bur hole/craniotomy is then planned using CT angiography–based neuronavigation, and overlies the selected recipient vessel in immediate proximity to the chosen donor vessel.
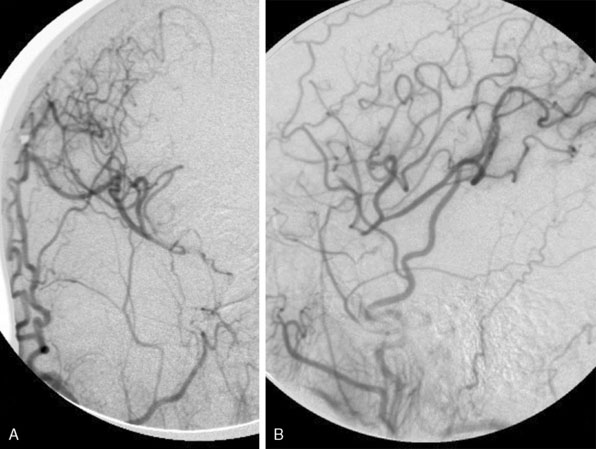
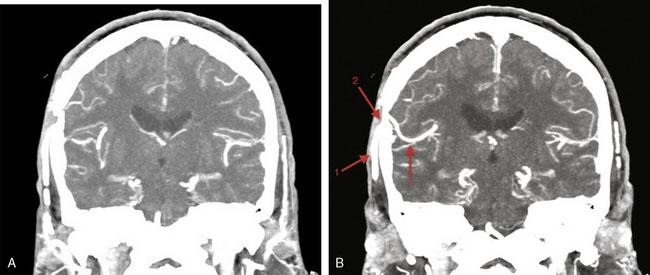
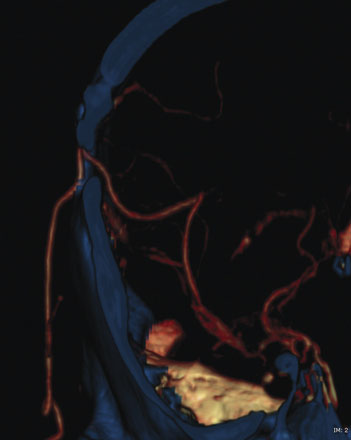
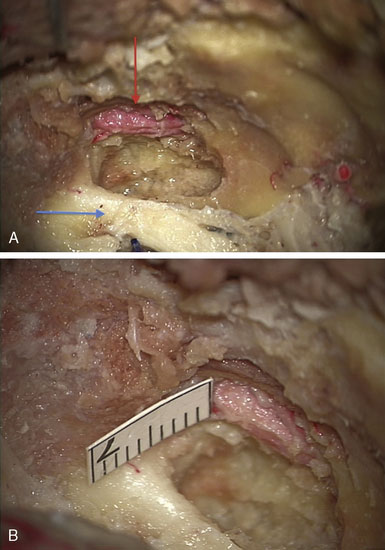
The incision is performed under the microscope where the temporalis muscle is split vertically directly below the selected donor branch of the STA. A bur hole is made and enlarged to the size of a small craniotomy (∼2 to 2.5 cm) under the microscope, and then 1 cm of the recipient vessel is exposed in the Sylvian fissure (Figures 15–2 and 15–3). A rubber dam is applied and the anastomosis is performed with a 9-0 nylon suture in a running fashion. The back wall is anastomosed before the front wall. Temporary clips are applied on the recipient vessel, the M4 branch of the MCA, during the anastomosis. Postoperatively, the patients were followed up with angiography or CT angiography, and clinically, disease progression was halted (Figures 15-4 through 15-7).

Figure 15–2 Intraoperative photograph obtained through the microscope while the bur hole/craniotomy was being performed.
(From Coppens JR, Cantando JD, Abdulrauf SI, Minimally invasive superficial temporal artery to middle cerebral artery bypass through an enlarged bur hole: the use of computed tomography angiography neuronavigation in surgical planning, J Neurosurg 2008;109(3):553–558, with permission.)

Since the publication of this minimally invasive procedure, Fischer et al.2 have described a similar minimally invasive procedure with the use of 3D virtual planning with the Dextroscope and magnetic resonance angiography in place of intraoperative stereotaxy that could serve as an alternative to the technique described above.
Minimally invasive high-flow bypass technique: internal maxillary artery to middle cerebral artery ec-ic bypass
High-flow cerebral revascularization currently requires graft vessel harvesting, cervical incision for the proximal anastomosis, craniotomy for distal anastomosis, and parent vessel occlusion. This conventionally necessitates a large craniotomy and extensive cervical incision. Instead, we illustrate a technique that avoids a long cervical incision and allows for purely intracranial extradural access to the internal maxillary artery (IMAX) to perform a short segment high-flow anastomosis from it to the MCA, using a radial artery graft.3
In recent years a number of important variations have been introduced to make the high-flow EC-IC bypasses less invasive. The contributions of C. A. F. Tulleken in devising the non-occlusive, laser-assisted anastomosis have to be commended (see Chapter 14). A case report was published using the Cardica C-Port xA Distal Anastomosis System for an automated high-flow bypass. This involves an automated end-to-side anastomosis with simultaneous arteriotomy and insertion of 13 microclips into the graft and recipient vessels. This latter technique however, is very limiting because of the size and configuration of the device and is unlikely to be used widely due to this important limitation.4
In this section we describe our development of the IMAX-MCA bypass technique, which we believe is much less invasive than the standard high-flow EC-IC bypass. Prior to clinical application of our bypass, we performed a series of six adult cadaveric dissections. The IMAX was dissected via a middle fossa extradural approach in the cadaveric specimens in order to confirm the middle fossa surface landmarks, location, and depth of the artery (Figure 15–8). This methodology was subsequently implemented in a clinical case as outlined below.
< div class='tao-gold-member'>
Related posts:
 Using Cerebral Vaso-Reactivity in the Selection of Candidates for EC-IC Bypass Surgery
Using Cerebral Vaso-Reactivity in the Selection of Candidates for EC-IC Bypass Surgery
 Radial Artery Harvest for Cerebral Revascularization: Technical Pearls
Radial Artery Harvest for Cerebral Revascularization: Technical Pearls
 EC-IC Bypass Evidence
EC-IC Bypass Evidence
 Bypass Surgery for Complex MCA Aneurysms
Bypass Surgery for Complex MCA Aneurysms
 EC-IC and IC-IC Bypass for Giant Aneurysms Using the ELANA Technique
EC-IC and IC-IC Bypass for Giant Aneurysms Using the ELANA Technique
 Decision Making in Cerebral Revascularization Surgery Using Intraoperative CBF Measurements
Decision Making in Cerebral Revascularization Surgery Using Intraoperative CBF Measurements
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


