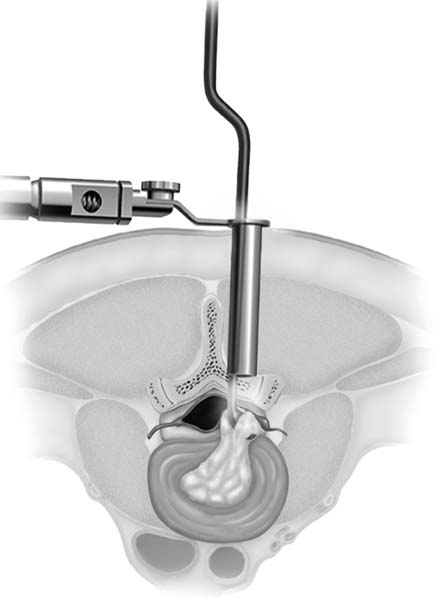
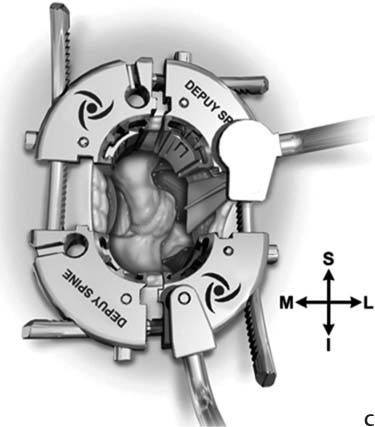
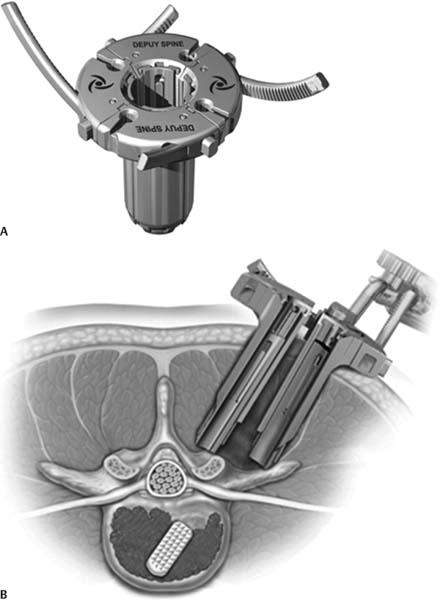
12 Advancements in spinal surgery during the last century have been significant. Whereas complex spinal fixation was previously performed only in select centers in the early 1980s, it is now commonplace in the majority of medical centers. The growth of the field has been driven by new technologies. This includes high-quality digital fluoroscopy, which has allowed a tremendous expansion in minimally invasive spinal (MIS) techniques. MIS techniques have significant advantages because they approach the spine through a smaller corridor of dissection, leading to less iatrogenic injury and less disruption of the musculoligamentous complex. Open procedures produce significant soft tissue injury, and it has been observed that the retractors used for posterior lumbar exposures exert significant pressure on the musculature, thereby inducing ischemia.1 Even short procedures, such as microdiskectomy, have been shown to lead to a 30% decrease in lumbar isokinetic strength with flexion.2 See and Kraft provided further evidence with electrophysio-logical studies showing chronic denervation and electromyographic (EMG) changes in the paraspinal muscles after open surgery.3 Radiographically, this has been demonstrated by significant long-term atrophy of the operated muscle segment.4 Sihvonen et al have directly correlated the degree of iatrogenic paraspinal injury with the increased incidence of failed back syndrome.5 MIS techniques avoid iatrogenic injury of the posterior musculoligamentous complex. As a result, there is decreased postoperative pain, shorter hospital stays, and improved recovery times.6–10 This chapter summarizes some of the tools/instrumentation systems used to perform MIS procedures on the spine. There are many MIS options available to the surgeon for access and stabilization of the spine. Helping to decipher the relative advantages of the various systems is the goal of this chapter. The push to make surgery less invasive and to minimize damage to normal tissue structures is a common goal throughout all surgical disciplines. Starting with Yasargil’s pioneering use of the operating microscope to perform a lumbar diskectomy in 1967, MIS surgery has had a renaissance in recent years due to the development of modern tubular retractor systems, which can be incorporated into almost any traditionally open procedure.11 These retractors allow surgeons to trade the large incisions and working spaces of open surgery for small (15 to 30 mm) incisions and targeted working spaces via narrow metal channels. In 1991, Wolfhard Caspar utilized a speculum-like retractor that can be considered a precursor to many of the current MIS tubular retractor systems to perform his variation of microsurgical diskectomy.12 Foley and Smith introduced and popularized what can be considered the first muscle-splitting, tubular-based retraction procedure, dubbed microendoscopic diskectomy (MED), in 1997. The initial system (MED tubular retractor, Medtronic, Minneapolis, MN), was an endoscopic procedure and did not gain significant support in clinical practice due to the steep learning curve of mastering endoscopic surgery.13 However, in 2003 the introduction of a tubular retractor system (METRx, Medtronic, Minneapolis, MN) that allowed surgeons to use the operating microscope led to popularization of tube-based procedures. Over the past decade, tubular retractors have grown in their complexity to become highly sophisticated devices incorporating expandable parts or skirts, fiberoptics, and endoscopic visualization options to aid in the performance of more complex surgical procedures. Each of these retractors allows for a muscle-splitting approach to the spine and thus significantly less destruction of the muscular anatomy and less soft tissue retraction. Multiple investigators have demonstrated that this leads to shorter hospital stays and diminished postoperative pain.14–16 There are several different MIS access systems available in the marketplace for surgeons to choose from. What follows is a comparative analysis of various commonly used tubular retractors (fixed and adjustable). Pros: • Versatility—can be employed in cervical, thoracic, and lumbar procedures. • Allows for direct visualization. • Decreases muscle damage and tissue disruption. • Unilateral bevel allows better medial visualization. Cons: • Definite learning curve in using system optimally. • Small working area risks inadequate decompression in some cases. The METRx tubular retractor (Medtronic, Minneapolis, MN) is the first tubular retractor system designed to split muscles along the path of insertion, thereby reducing tissue trauma. After K-wire placement and incision, a working corridor is developed by serial dilation (Fig. 12.1). The great versatility of the METRx system has lent itself to use in the cervical, thoracic, and lumbar spine with predominantly posterior applications but some anterior applications as well. While the strength of the system is in facilitating MIS microdiskectomy, laminectomy, or other microscopic decompression procedures, the METRx system has been used for instrumentation with screws and rods in the cervical spine, albeit with an increased difficulty of placing rods through the small working channel.17 The second-generation design of this retractor incorporates a bevel on one side of the working space to facilitate medial exposure. It is not recommended to use fixed-diameter tubular retractors for centralized thoracic disk herniations because the rigid wall of the tubular retractor limits the lateral angulation of instruments needed to safely work under the spinal cord to avoid injury. Fig. 12.1 Illustrated cross-section showing the METRx (Medtronic, Minneapolis, MN) tubular retractor passing through the paraspinal muscles and docking above the intervertebral space following successful placement. The tubular retractor is stabilized via an articulating arm affixed to the operating table. (Courtesy of Medtronic.) Pros: • Built-in light source improves visualization without use of the operating microscope. • Versatility—can be employed in cervical, thoracic, and lumbar procedures. • Allows for direct visualization. • Decreases muscle damage and tissue disruption. Cons: • Limited visualization at the base from fixed circular design. • Definite learning curve in using system optimally. • Small working area risks inadequate decompression in some cases. • Rigid wall increases risk of cord injury when performing thoracic diskectomy unless the disk is very lateralized. The Spotlight Access System (DePuy Spine, Inc., Raynham, MA) access system is a dilator-based tubular retractor very similar to the METRx system. It incorporates a built-in light source that can help eliminate shadows at the base of the working channel (Fig. 12.2). The fixed circular end of the working channel does limit visualization somewhat. Pros: • Radiolucent retractor facilitates improved fluoroscopic imaging. • Additional cannulas can be used to expand working area. • Expansive workspace allows for facile posterolateral fusions. Cons: • Standard drawbacks of other fixed tubular retractors. The Vuepass (Biomet, Parsippany, NJ) is one of the most recently introduced MIS access technologies. The unique feature of Vuepass is that it is constructed from Makrolon, a polycarbonate thermoplastic polymer. This design choice makes it radio-lucent on fluoroscopy, and makes it possible to view structures that may be obscured by the retractor while one is using fluoroscopy. In addition, Vuepass incorporates many of the features of other systems. Larger-diameter cannulas can be added to span more than one level and permit both interbody and posterolateral fusions, as well as other standard procedures. Its radiolucency, in addition to its other features and compatibility with any screw–rod system, make the Vuepass a versatile retraction system. Fig. 12.2 Rendering of the integrated light source on the distal end of the Spotlight (DePuy Spine, Inc., Raynham, MA) tubular retractor. The light source can enhance direct visualization, but its utility is somewhat limited by the decreased visibility from the tube’s restrictive circular geometry. (Courtesy of DePuy.) Pros: • Versatility—can be employed in cervical, thoracic, and lumbar procedures. • Reduced muscle damage and tissue disruption. • Expandable base significantly increases work area compared with METRx. • Optional integrated light source. Cons: • Expanded work area leads to greater tissue disruption. • Muscle damage from overuse of monopolar coagulation. The X-TUBE (Medtronic) is the evolution of METRx to incorporate an expandable workspace at the base of the retractor. The base can expand from 2.6 to 4.4 cm; the X-TUBE is mainly employed for performing transforaminal lumbar interbody fusion (TLIF) and posterior lumbar interbody fusion (PLIF) procedures. After K-wire placement, an incision is made and a series of tubular dilators are used to develop the working channel. Once the dilators are in place, the X-TUBE is placed over them and held in place by an articulated arm affixed to the table. Interbody fusion can be performed through the closed X-TUBE, after which the X-TUBE can be expanded to give direct visualization between adjacent pedicles in most patients. This allows for direct placement of pedicle screws and rod as well as intratransverse arthrodesis, if desired. For multilevel fusions, the X-TUBE requires multiple placements and, due to the increased operative time this can cause, for fusions exceeding three or more levels, it may be preferable to utilize an alternative approach (lateral or open). Pros: • Expands internally to span up to two segments, thereby only requiring a small incision on each side of the spine. • Direct visualization throughout procedure via expandable retractor with skirt. • Allows for interbody fusion, posterolateral fusion, and direct screw and rod placement. • Can be used for two-level fixation. Cons: • Less rigid wall requires extensive mobilization of tissue off the spine to optimize retraction that can lead to increased muscle damage and postoperative pain/spasm. The FlexPosure® Portal (Zimmer, Minneapolis, MN) MIS system, sold as a complete rod and screw system as TiTLE 2® (Zimmer), is an MIS system built around a unique visualization device. Unlike other MIS systems, the FlexPosure® Portal incorporates a unique expander with a flared “skirt” at the base and a pivoting upper cannula that allows direct visualization of up to two levels of the spine (Fig. 12.3). This expansive range of vision permits completion of a two-level fusion performed through a small incision under direct visualization. The drawback to this method is that more extensive tissue dissection is required, thereby causing a greater perturbation of normal anatomical structures. Additionally, large multilevel fusion constructs require multiple placements of the FlexPosure® Portal retractor and therefore can take more time when compared with other approaches. Pros: • Individually telescoping blades help prevent muscle creep. • Curved retractor skeleton increases distal visualization while minimizing superficial exposure. Fig. 12.3 Illustration of the FlexPosure® Portal (Zimmer, Minneapolis, MN) demonstrating its expanded viewing field and flared skirt. The lower panel demonstrates the simultaneous visualization of multiple levels via a single incision. Fig. 12.4 (A) Illustration of the Pipeline system (DePuy Spine, Inc., Raynham, MA) showing its individually telescoping blades fully retracted. (B) Axial view of final medial-lateral positioning of the dilator through the multifidus and longissimus muscles. (C) The retractor blades are opened, providing an expansive view of an exposed facet joint. (Courtesy of DePuy.) • Can be expanded independently in both cephalad-caudal and medial-lateral directions to simultaneously visualize up to two levels. • Comes in both large and small sizes and accommodates a light source. Cons: • Slightly complicated assembly. • Requires larger superficial incision than other expandable retractors. Pipeline (DePuy Spine, Inc., Raynham, MA) was designed primarily for posterior lumbar decompression and instrumented arthrodesis (Fig. 12.4A–C
Minimally Invasive Instrumentation Systems
Minimally Invasive Access/Tubular Retractor Systems
Background
Select Minimally Invasive Spinal Access Systems
METRx Tubular Retractor (Medtronic)
Spotlight Visualization System (DePuy)
Vuepass (Biomet)
X-TUBE Dynamic Visualization System (Medtronic)
FlexPosure®Portal Visualization System (Zimmer)
Pipeline Expandable Access System (DePuy)
Related posts:
 Promising Advances in Minimally Invasive Spine Surgery
Promising Advances in Minimally Invasive Spine Surgery
 Minimally Invasive Lumbar Diskectomy
Minimally Invasive Lumbar Diskectomy
 Minimally Invasive Transforaminal Lumbar Interbody Fusion
Minimally Invasive Transforaminal Lumbar Interbody Fusion
 Minimally Invasive Lumbar Interbody Fusion: Choosing Between Approaches
Minimally Invasive Lumbar Interbody Fusion: Choosing Between Approaches
 Minimally Invasive Lumbar Laminectomy for Stenosis
Minimally Invasive Lumbar Laminectomy for Stenosis
 Alternative Approaches for Lumbar Fusion: Axial Lumbar Interbody Fusion (AxiaLIF)
Alternative Approaches for Lumbar Fusion: Axial Lumbar Interbody Fusion (AxiaLIF)
![]()
Stay updated, free articles. Join our Telegram channel



Full access? Get Clinical Tree


