The decision to operate on the patient with a missile injury to the brain requires careful consideration of the mechanism (gunshot wound, shrapnel, blast injury, etc.), the patient’s pre- and post-resuscitation Glasgow Coma Scale (GCS), and specific imaging findings (Fig. 71.1).
♦ Preoperative
- Careful assessment of the extent of injury including identification of all wounds, extent of skin damage, and proximity to dural sinuses
- Administration of tetanus vaccination
- Seizure prophylaxis, typically phenytoin or fosphenytoin load, 18 mg/kg
- Antibiotic prophylaxis with broad spectrum agent with good central nervous system penetration (e.g., ceftriaxone 1 to 2 g based on weight)
Operative Planning
- Goals of surgery areas follows:
- Débridement of devitalized tissue
- Removal of hematoma causing mass effect
- Removal of accessible bone fragments and foreign bodies (it is not necessary to remove inaccessible fragments at the expense of viable brain tissue)
- Hemostasis
- Adequate closure of dura if possible (autologous graft should be considered)
- Meticulous closure of galea and scalp
- Débridement of devitalized tissue
- Placement of external ventricular drain or intraparenchymal intracranial pressure (ICP) monitor in patients with GCS ≤ 8
< div class='tao-gold-member'>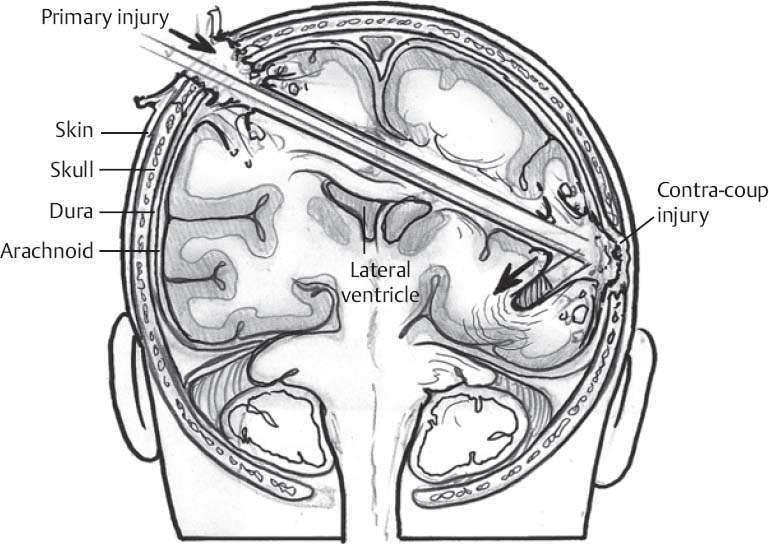 Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


