CHAPTER 14 MRI Evaluation of Meningiomas
INTRODUCTION
Magnetic resonance imaging (MRI) is the state of art in the preoperative diagnosis of meningiomas. The diagnostic accuracy of standard MRI is approximately 95%. Further, contrast-enhanced MRI has the highest ability to detect and characterize meningiomas radiologically.1 This high rate of diagnostic accuracy can be attributed to special properties of the MRI technique presented in this chapter that provide vast information on meningiomas.
MRI OF THE DURA MATER RELATED TO MENINGIOMAS
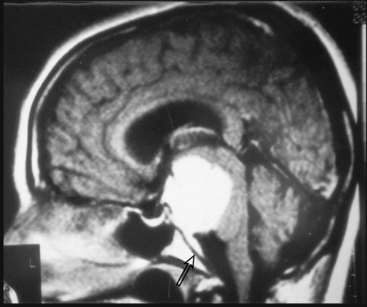
Meningiomas arise from the meningothelial cells of the arachnoid membranes, which are attached to the inner layer of the dura mater. This close relationship between the meningioma and the dura mater can be demonstrated on MR imaging. Normal dura mater is a non-neuronal connective tissue and appears as a hypointense thin layer adjacent to the hypointense inner table of bone on T1- and T2-WI (Fig. 14-1). After contrast injection, dura and the dural reflections of falx cerebri, tentorium, and cavernous sinus enhance as a thin discontinuous layer (Fig. 14-2).2 The demonstration of the dura mater and the adjacent meningioma on MRI supplies information about the extra-axial location and the origin of meningioma. In this respect, MRI is advantageous over computed tomography (CT) imaging, in which bone and enhanced dura both appear as hyperdense structures and cannot be distinguished from each other. The sensitivity of MRI is two to three times higher than that of CT for imaging dural and meningeal pathologies.3 Dural attachment of a meningioma is usually broad and the angle between the tumor and the dura is an obtuse one, indicating the extra-axial location of the meningioma (Figs. 14-2 and 14-3). Rarely the dural attachment may be narrow and a pedunculated meningioma can be demonstrated, more so in cases with large subarachnoid spaces where the peduncle becomes more conspicuous.
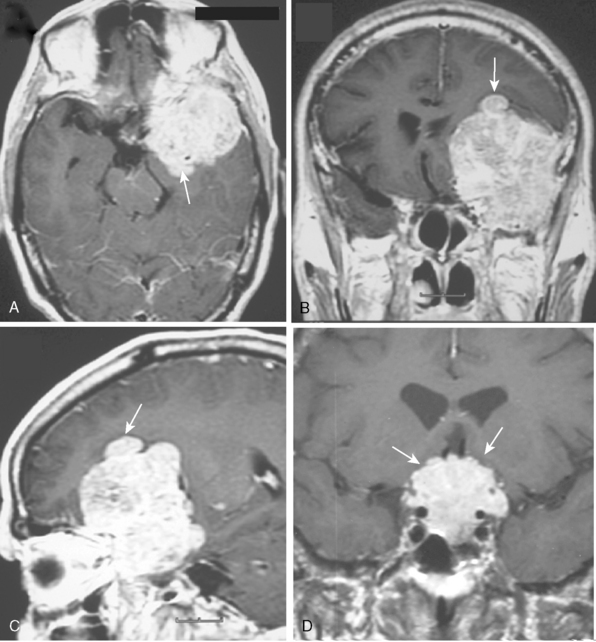
Pathologic enhancement of the dura mater and the adjacent inner table of bone, known as pachymeningeal enhancement, may be due to abnormally increased capillary permeability, increased blood volume, edema, tumor invasion of the dura mater, or as a result of surgery.2 The local pachymeningeal enhancement adjacent to a meningioma which tapers smoothly away from the tumor is designated as a dural “tail” (Fig. 14-4). The dural “tail,” which is depicted radiologically only on MRI, is reported in 52% to 72% of meningiomas. Nevertheless, it is nonspecific, and has also been associated with lymphomas, sarcoidosis, schwannomas, metastatic tumors, syphilitic gumma, and hemangiopericytomas.4–10 A dural “tail” may also be demonstrated, without contrast injection, on MR FLAIR sequences. Both meningiomas and the dural “tail” are demonstrated on FLAIR sequences, yet the dural “tail” usually has higher signal intensity than the tumor.11
MRI FINDINGS SUPPORTING EXTRA-AXIAL LOCALIZATION OF MENINGIOMAS
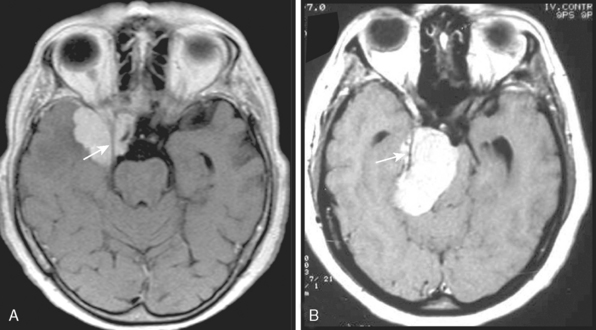
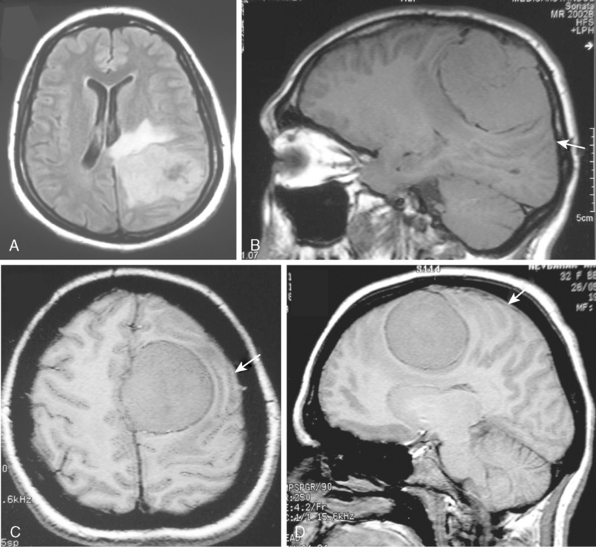
The extra-axial localization of a mass is an important diagnostic finding, albeit it is not always simple to appreciate this finding, more so when a dural relation cannot be detected (Fig. 14-5). A cerebrospinal fluid (CSF) interface between a mass and the brain surface is another finding supporting the extra-axial localization (Fig. 14-6). Occasionally the subarachnoid space around a meningioma may enlarge and acquire the form of a cyst. Another finding reflecting the extra-axial localization of a meningioma is the “buckling” or compression and displacement of adjacent brain cortex and the white matter (Fig. 14-7).
BORDER AND CONTOUR OF MENINGIOMAS
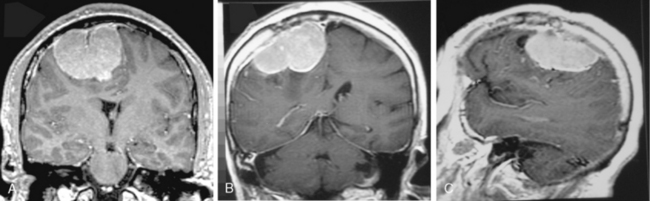
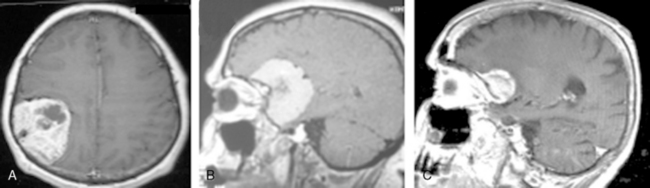
The borders and contours of meningiomas are usually regular and the margins are sharp as a result of the extra-axial location of the tumor which is surrounded by a CSF ring (Fig. 14-8). Despite the extra-axial location, meningiomas may indent into the adjacent brain cortex and so exhibit irregular margins. A meningioma that has multiple lobulated outgrowths on its contour is designated as “mushrooming” meningioma (Fig. 14-9).
CONTRAST ENHANCEMENT OF MENINGIOMAS ON MRI
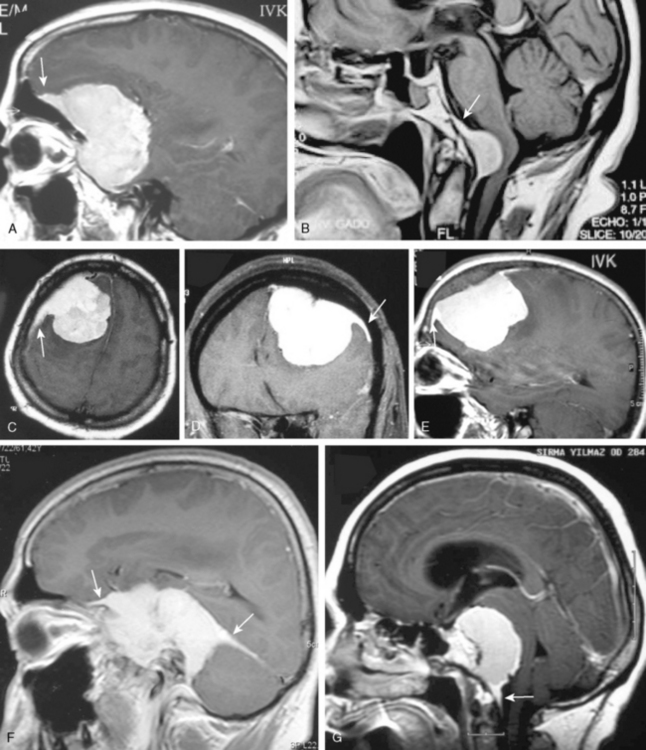
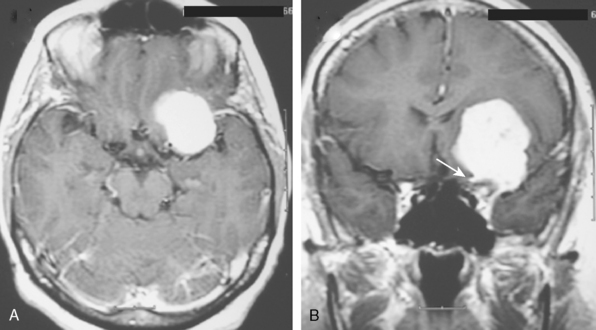
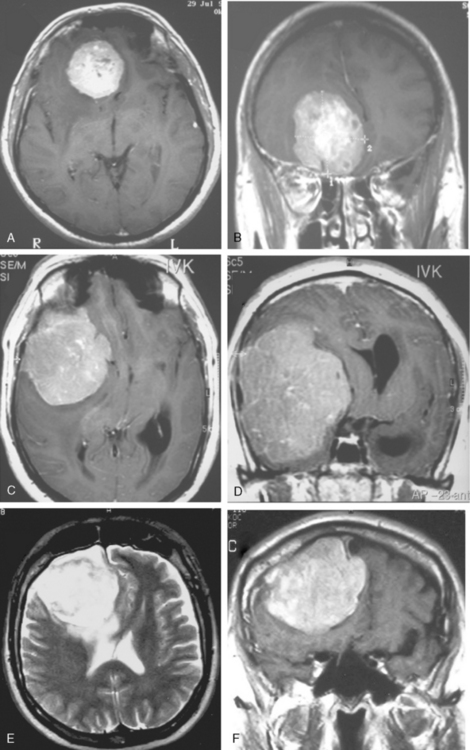
MRI contrast agents are gadolinium chelates that shorten the T1 relaxation times in certain tissues to increase signal intensity on T1-WI and produce contrast enhancement that improves the sensitivity of MRI for residual, recurrent, and multiple meningiomas.12 On early MR studies, some small meningiomas with signal intensities close to that of the brain cortex on T1- and T2-WI were not recognized if contrast medium was not used.1 Routine use of contrast media is necessary to increase the sensitivity for meningioma detection. Meningiomas that are homogeneous on T1-WI and T2-WI enhance in general intensely and in a uniform manner (Fig. 14-10). Calcified, cystic, necrotic, and hemorrhagic meningiomas enhance less intensely, and more heterogeneously (Fig. 14-11). No correlation was established between contrast enhancement and the histopathologic features of meningiomas.13 Contrast media are among strong radiodiagnostic tools; however, caution is recommended in patients with poor kidney functions, as cases of nephrogenic systemic fibrosis have been related to some ingredients of MR contrast agents.
EDEMA RELATED TO MENINGIOMAS ON MRI
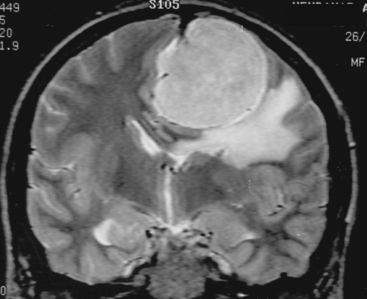
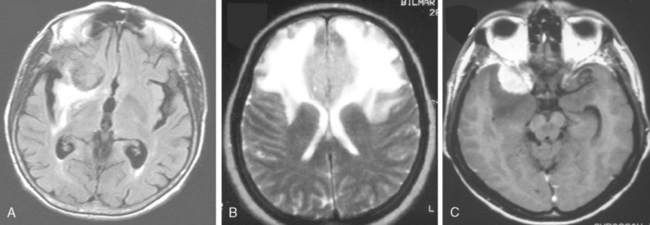
Despite their extra-axial location, meningiomas can cause mild to extensive vasogenic white-mater edema in up to 75% of cases.14 Calcified meningiomas exhibit less vasogenic edema.15 Many factors were associated with the development of edema. These include shape of meningioma, mechanical injury to the adjacent brain tissue, compression of nearby vasculature, angiogenic factors, large surface area of the tumor, invasive pattern of brain–tumor interface and hyperintensity of meningioma on T2-WI.14–16 Nevertheless, the exact cause of edema is still unknown. Newer techniques such as diffusion tensor imaging may provide additional information. Vasogenic edema in the white matter presents in the form of “finger edema” and is hypointense on T1-WI, and of hyperintense and of homogeneous signal intensity on FLAIR and T2-WI (Fig. 14-12). Small and isointense meningiomas amid edema can be depicted only after contrast medium administration.
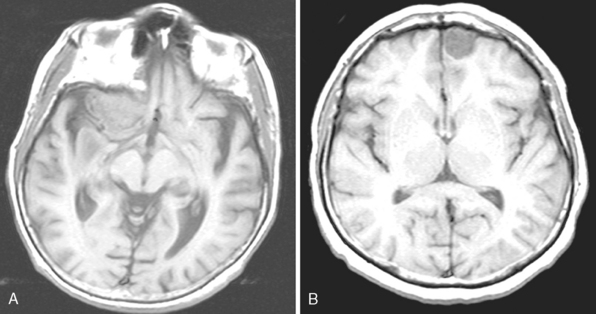
MR SIGNAL INTENSITY CHARACTERISTICS OF MENINGIOMAS
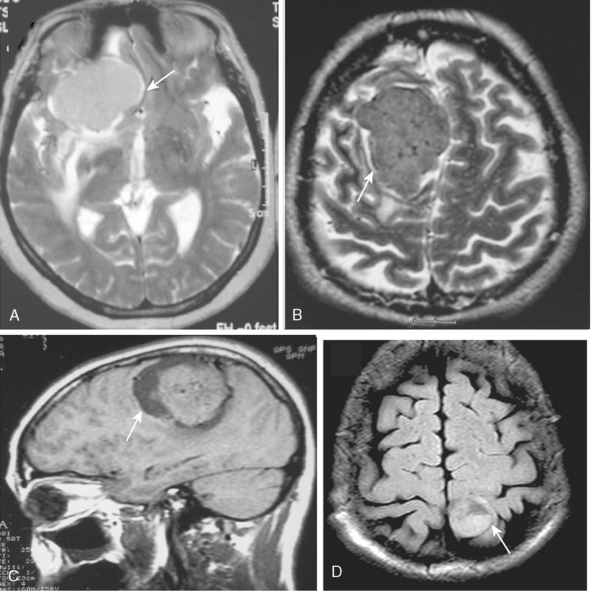
Signal intensity characteristics of meningiomas have been studied extensively and correlated with the histologic subtypes of meningiomas. According to Elster and colleagues, in 62% of meningiomas, the signal was isointense with cortical gray matter, and in the remaining 38% hypointense to gray matter intensity on T1-WI so that no correlation could be established concerning the histologic type on T1-WI (Fig. 14-13).17 On proton density (PD) and T2-WI meningiomas are isointense in 50% and mildly hyperintense to cortex in 40% of cases (Fig. 14-14).18 Signal intensity of meningiomas on T2-WI could be correlated to histologic subtypes in 75% of cases, so that varied MR findings may be explained on a histologic basis.17 Fibroblastic meningiomas with a dense collagenous matrix produce hypointense signal on T2-WI (Fig. 14-15). Transitional meningiomas with abundant psammoma bodies have relatively low signal intensity on T2-WI (Fig. 14-16). Syncytial meningiomas with microcystic elements exhibit high signal intensity on T2-WI (see Fig. 14-11E, F).13 Angioblastic meningiomas with high cellularity and dilated blood vessels show hyperdense signal with a mottled appearance on T2-WI (Fig. 14-17).13






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


