Cancer is the second leading cause of death in persons over 65 years of age. In 2006, it was estimated that 782,482 Americans over 65 years of age were diagnosed with cancer and 397,640 persons in that age group died of the disease (53). With the shift in demographics to a larger percentage of elderly and with improved prevention and treatment of heart disease and stroke, elderly patients with cancer will become even more prevalent in the new century. As many as 20% to 25% of patients with systemic cancer harbor intracranial metastases at the time of death, and 5% of patients with systemic cancer develop epidural cord compression during the course of their illness. Applying these percentages to the statistics noted above indicates a very large number of patients presenting to their physicians with neurologic signs and symptoms directly related to their systemic malignancies.
Although primary CNS tumors currently account for <2% of all malignancies in the elderly, their frequency has increased steadily over the last three decades (25). The American Cancer Society estimates that 18,820 persons were diagnosed with primary CNS cancer in 2006 (patients >65 years old accounted for an estimated 35% of these cases) and 12,820 persons died from these tumors in that year (48% of those dying were 65 years or older) (53). Some studies have estimated the increase in incidence of primary brain tumors in patients over 65 years of age to be from 15% to 500% over the last 20 years (28,30,37). The increased incidence is particularly pronounced in the extreme elderly (≥85 years). The cause of this troubling increase is unclear. It may be caused, at least partially, by the widespread availability of sophisticated neuroimaging and increased access to specialized medical care for the elderly over the last 30 years. These advances alone, however, do not fully account for this trend. The incidence of primary malignant brain tumors started to rise even before the introduction of computed tomography (CT) scanning in the early 1970s, and the trend has continued to increase even since the 1980s, when CT scanning capability became standard in most medical facilities (65).
Neuro-oncology is the study of cancer’s effects on the central and peripheral nervous system. This includes direct involvement of the nervous system by tumor and so-called “remote effects,” which broadly include paraneoplastic disorders, cerebrovascular complications, infections, and toxic or metabolic disorders that can be secondary effects of cancer or its treatment. Table 28-1 lists the various categories of neurologic illness seen in patients with cancer.
This chapter focuses on the primary and metastatic tumors of the brain and spinal cord most commonly seen in the older adult. A section in this chapter outlines the well-described, although rare, paraneoplastic neurologic disorders.
CLASSIFICATION
Brain and spinal tumors can be broadly classified as either primary (tumor arising from cells of the brain and spinal cord or their coverings) or metastatic (tumor spread from other primary sites within the body). By definition, metastatic tumors are always malignant. Primary tumors can be benign or malignant, depending on the underlying histopathology. Overall, metastatic tumors are the most common brain tumors seen in elderly patients. However, in a patient presenting with a new, solitary brain neoplasm and no history of systemic cancer, a primary tumor is the more likely diagnosis.
Among primary brain tumors, most series suggest that meningioma is most common, followed by malignant (high-grade) glioma, pituitary adenoma, schwannoma (including acoustic neuroma), low-grade glioma, and primary central nervous system (CNS) lymphoma (PCNSL).
METASTATIC TUMORS
BRAIN METASTASES
Among older adults, metastatic tumors are more common than primary brain tumors, occurring in 20% to 25% of all patients dying of cancer, based on autopsy series (36,47,50). The incidence is less common in clinical series in which primarily symptomatic brain lesions will usually be included (56,64). Virtually any malignant systemic tumor can metastasize to the brain. Breast and lung cancers are the most common systemic tumors and, therefore, account for most brain metastases. Some less common malignancies have a special proclivity to metastasize to the brain. Thus, although melanoma accounts for only 4% of systemic tumors, it has accounted for as much as 10% of brain metastases, and as many as 40% of patients with melanoma were found to harbor brain metastases at autopsy (1). Small-cell lung cancer is more than twice as likely to metastasize to the brain as other types of lung cancer.
Table 28-1.Neurologic Illnesses in Patients with Cancer
Direct tumor involvement
Infection
Brain or cord parenchymal metastases
Listeria monocytogenes
Meningeal metastases
Cryptococcus neoformans
Dural metastases
Aspergillus fumigatus
Epidural metastases
Mucor
Plexus metastases
Herpes zoster
Peripheral nerve metastases
JC virus
Toxic metabolic disorders
Cytomegalovirus
Liver or renal disease
Toxoplasmosis
Electrolyte disturbances (SIADH)
Adverse effects of therapy
Hypercalcemia
Radiation encephalopathy
Hypomagnesemia
Radiation myelopathy
Hypothyroidism
Radiation plexopathy/radiculopathy
Chemotherapy toxicity
Chemotherapy-induced encephalopathy
Opioid toxicity
Chemotherapy-induced neuropathy
Corticosteroid toxicity
Steroid psychosis
Vascular disorders
Steroid myopathy
Nonbacterial thrombotic endocarditis
Phantom limb syndrome
Disseminated intravascular coagulation
Postmastectomy pain syndrome
Hyperviscosity syndrome
Postthoracotomy syndrome
Thrombocytopenia
Paraneoplastic syndromes
Hypercoagulable state
Lambert-Eaton myasthenic syndrome
Dural sinus thrombosis
Myasthenia gravis
Tumor embolus
Paraneoplastic cerebellar degeneration
Tumor hemorrhage
Paraneoplastic limbic encephalitis
Paraneoplastic sensory neuropathy
Opsoclonus-myoclonus syndrome
Polymyositis/dermatomyositis
SIADH, syndrome of inappropriate antidiuretic hormone.
Some evidence indicates that the incidence of metastatic brain tumors is increasing (47,50). This is likely caused by a combination of factors: (a) sophisticated neuroimaging allows diagnosis of brain metastases even at an asymptomatic stage; (b) improved treatment of the systemic cancer means that patients are living longer and have more opportunity to develop brain metastases; and (c) the CNS appears to be a “sanctuary” from the effects of chemotherapy, allowing brain metastases to grow, even when systemic tumor is controlled.
The pathogenesis is hematogenous tumor spread in most patients. In more than 50% of cases, the lesions are multiple. The “watershed” region of the cerebral hemispheres is the most likely site of metastases, and the corticomedullary junction is the most common point of origin (15). These pathologic data suggest that arterial tumor microemboli lodge in the distal capillary arcades of the cerebral arteries. Supratentorial metastases are distinctly more common than infratentorial (90% vs. 10%) in patients with breast and lung cancer. The metastases are more evenly divided between the supra- and infratentorial compartment in patients with colon cancer and uterine cancer. This suggests a possible role of metastasis via the Batson venous plexus, although some studies refute that hypothesis (15,42).
Clinical Presentation
Most brain metastases (80%) occur in patients in whom the diagnosis of systemic malignancy is already established. The clinical presentation varies considerably among individuals and largely depends on the location of the brain metastasis or metastases. In younger patients, the most common symptoms are headache and seizure. Among elderly patients, focal deficits (e.g., hemiparesis and aphasia) and cognitive changes are distinctly more common, perhaps because older brains have more atrophy and room to accommodate an expanding mass lesion. It is not clear why elderly patients are less likely to present with seizures. Perhaps the seizure threshold of the elderly brain is higher.
Not infrequently, elderly patients with brain metastases are misdiagnosed as having a “stroke.” This is especially common in patients who do not have a previous diagnosis of a primary tumor or in those who present with very acute symptomatology. Focal seizure and tumor hemorrhage can both masquerade clinically as a stroke. The diagnosis usually is not difficult if a careful history is taken and neuroimaging is interpreted appropriately.
Diagnosis
A CT of the head with contrast is sufficient in most cases to make the diagnosis of brain metastases, although magnetic resonance imaging (MRI) of the head has become standard for diagnosis in most centers. CT is less expensive than MRI and easier to perform on a patient who is confused or uncooperative. In patients whose condition is deteriorating rapidly, CT is adequate to diagnose secondary conditions such as obstructive hydrocephalus and tumor hemorrhage. Extra care must be taken in elderly patients to ensure that their renal function is adequate to handle the iodinated contrast. Approximately 5% of patients will have an allergic reaction to the iodinated contrast dye, and the dye can precipitate focal seizures in as many as 10% of patients with brain metastases (2). MRI with contrast is more sensitive, particularly for small brain metastases. It is also more expensive and requires better patient cooperation.
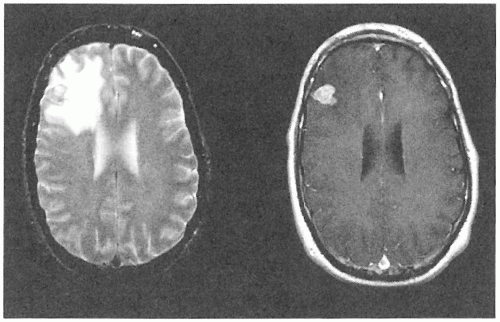
Both CT and MRI demonstrate enhancing lesions, typically with central necrosis. Metastases are usually multiple, which can be better appreciated on MRI when the lesions are tiny. Typically in brain metastases, the lesions are well circumscribed and have a disproportionate amount of edema than expected for the size of the enhancing lesion (Fig. 28-1). These features may help distinguish them radiographically from primary brain tumors, which tend to be more diffuse and have a pattern of edema that more closely approximates the area of enhancement. A brain abscess may mimic the appearance of metastasis, although brain abscesses are rare unless the patient is immunocompromised.
Figure 28-1. Brain metastasis. Axial MRI of the head: T2-weighted image (left) and T1-weighted image with gadolinium contrast (right). Note the large amount of edema compared to the lesion’s size.
In patients who have known metastatic systemic cancer, the diagnosis is generally made radiographically, and pathologic confirmation may not be required before treatment. The situation is more problematic in patients without a known systemic malignancy. If the radiographic picture is suggestive of metastatic tumor, a careful search for systemic malignancy should be undertaken. This begins with a thorough physical examination, followed by appropriate blood tests and imaging procedures [body CT, mammography, positron emission tomography (PET) scan]. Lung, breast, skin, renal, and gastrointestinal system are the most common sources of a primary malignancy in these cases. If no primary tumor can be found, then surgical biopsy or resection of one of the brain lesions is appropriate to make a diagnosis.
Treatment
Although the approach to treatment can vary, depending on the individual patient and type of malignancy, some interventions apply to all patients. Corticosteroids reduce peritumoral edema and can significantly reduce headache from raised intracranial pressure and may improve neurologic deficits produced by tumor mass effect. Approximately 30% to 40% of patients with brain metastases will have seizures at some point in their illness. This figure is higher among patients with hemorrhagic metastases and those with metastatic melanoma, in whom it is >50% (10). Any patient who has had a seizure should receive anticonvulsants, as should patients with metastatic melanoma. Otherwise, prophylactic anticonvulsants are best avoided because they interact with corticosteroids and various chemotherapy agents. Both phenytoin and carbamazepine can cause Stevens-Johnson syndrome, particularly in patients receiving whole-brain radiation therapy (WBRT) (16). Moreover, no significant reduction in the incidence of seizures has been seen in patients who received prophylactic anticonvulsants (20).
Surgery In patients with multiple lesions, surgery is limited to those who lack a known primary tumor. In this situation, biopsy without resection is appropriate to make a pathologic diagnosis. More extensive surgery is indicated in selected situations. For instance, in a patient with a large cerebellar metastasis obstructing the fourth ventricle, a resection of the offending metastasis may be life saving and allow the patient to tolerate WBRT without brain herniation. Data suggest that patients who have a surgically accessible solitary metastasis (as proved on enhanced MRI) and limited systemic cancer survive longer with less neurologic disability if they have resection of their metastasis (46,61). Surgery is a further consideration in patients with a recurrent metastasis after WBRT has been administered or in those with tumors that are known to be radiation resistant.
Radiation Therapy WBRT is the mainstay of treatment for most patients with brain metastases. It prolongs survival but is not considered curative. WBRT after resection of a solitary metastasis has been demonstrated to reduce the risk of CNS recurrence and neurologic death but did not improve survival overall when compared to patients receiving surgical resection alone (45). Most patients with brain metastases will die of progressive systemic cancer, not brain disease. The treatment is given to ports encompassing the whole brain, to a total dose of 2,000 to 3,000 cGy in 10 to 15 fractions. More accelerated radiation schedules may be appropriate in very frail patients with a short life expectancy. WBRT is usually well tolerated. Radiation-induced tumor swelling is best managed with corticosteroids. If they survive more than 6 to 12 months, elderly patients can be particularly susceptible to develop radiation encephalopathy. This is characterized by subcortical dementia with gait apraxia and urinary incontinence. CT and MRI demonstrate cortical atrophy, hydrocephalus ex vacuo, and diffuse white matter changes. More localized radiation, including gamma knife and stereotactic linear accelerator therapy, is probably best reserved for small recurrent brain metastases. The value of these latter therapies in the primary treatment of brain metastases remains to be clearly established.
Chemotherapy Most chemotherapy agents do not penetrate the blood-brain barrier well. Historically, chemotherapy agents have little efficacy in the treatment of most types of brain metastases. The recent development of chemotherapy agents that penetrate the blood-brain barrier, including temozolomide, topotecan, and signal transduction inhibitors, holds some promise in the treatment of brain metastases (11).
Prognosis
Once brain metastases have developed, the patient’s cancer, with rare exception, has reached an incurable stage. Without treatment, life expectancy is usually less than 4 to 6 weeks, and most patients die from their neurologic disease in that setting. With radiation therapy, survival extends to a median of 3 to 6 months. Most treated patients will die of progressive systemic cancer, not of brain metastases. Long-term survival (>1 year) is exceedingly rare among elderly patients.
EPIDURAL CORD COMPRESSION
Tumor in the epidural space usually has spread from the adjacent vertebra. Vertebral metastases are common, occurring in 25% to 70% of patients with metastatic cancer. The thoracic spine is particularly susceptible because it makes up the largest bony mass of the spine. The solid tumors that most commonly metastasize to the vertebra are lung, breast, prostate, renal, and thyroid cancer. Myeloma is the most common hematopoietic tumor to produce epidural cord compression. Tumor can invade the epidural space through the intervertebral foramen, without direct invasion of bone. The latter mechanism is seen in lymphomas arising from the paraspinal lymph nodes. Clinical signs of epidural cord or cauda equina compression can develop in as many as 5% to 10% of patients with metastatic cancer (4).
Clinical Presentation
Pain, the most common initial symptom, is present in 95% of patients at presentation to the physician (24). The pain can derive from the bony vertebral involvement or from compression of spinal roots. Vertebral pain is usually sharp or dull, localized over the involved vertebra, and worse with activities that stress the spine, such as standing and twisting. Bone pain is typically worse at night. Radicular pain is sharp and lancinating and is distributed along the root’s cutaneous dermatome. Radicular pain can also be worse with movement and with Valsalva maneuvers. Bone and radicular pain often precede neurologic deficits by weeks or months.
Neurologic deficits can develop acutely or subacutely and depend on the spinal level of involvement. Epidural tumor in the cervical and thoracic region will produce a myelopathy with spastic limb weakness, sensory level to pain and temperature, and loss of bowel, bladder, and sexual function. Lhermitte phenomenon may occur in patients with epidural tumors in the cervical or thoracic region. Compression of the thecal sac below L1 will produce a cauda equina syndrome with flaccid paraparesis, saddle distribution sensory loss, and loss of bowel, bladder, and sexual function. Epidural cord and cauda equina compression constitutes a neurologic emergency. Once neurologic function is lost, it may not be regained, despite appropriate treatment. Diagnosis and treatment, therefore, should proceed as quickly as possible.
Diagnosis
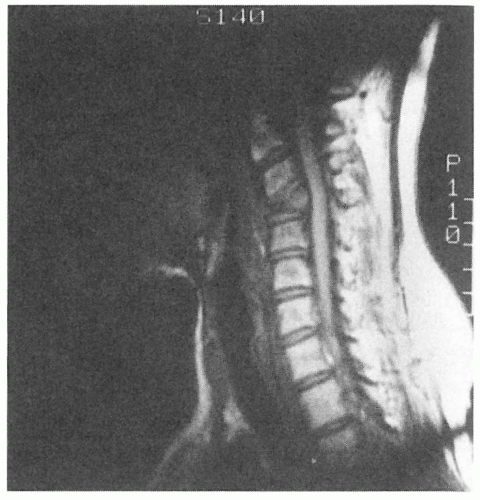
Although a plain X-ray study of the spine can identify the vertebral lesion in approximately 80% to 90% of patients with epidural tumor (48), it does not visualize the epidural space. MRI of the spine is superior in this regard and has largely replaced myelography, except for cases in which MRI cannot be performed (i.e., patients with cardiac pacemakers). MRI will demonstrate the level of vertebral and epidural involvement and confirm the presence of cord or cauda equina compression (Fig. 28-2). In addition to the spinal level of clinical interest, it is generally recommended that the entire spine be visualized with sagittal MRI views to rule out other levels of subclinical epidural involvement. As many as 30% of patients may have other levels of epidural involvement on MRI that are not suspected clinically (54).
Treatment
If epidural cord or cauda equina compression is clinically suspected, the patient should immediately be given high-dose intravenous corticosteroids. Dexamethasone (100 mg) is the treatment of choice. This reduces tumor swelling and spinal cord edema. It may prevent neurologic deterioration while the patient is awaiting diagnostic procedures and more definitive treatment. Corticosteroids provide analgesia for bone-related pain. Opioid analgesia should be given concomitantly for patients with moderate to severe pain. Side effects of high-dose steroids include manic psychosis, insomnia, and hyperglycemia. Hiccoughs are extremely common. If dexamethasone is given as an intravenous bolus, 50% of patients will experience intense but short-lasting perineal burning (5). This effect is self-limited, but patients should be warned before the steroids are given as a bolus.
Figure 28-2. Epidural cord compression from vertebral metastasis (lung primary). Sagittal MRI of the cervical spine: T2-weighted image without contrast showing malignant involvement of C3 vertebra with compression fracture and extension of tumor into the epidural space with compression of the cord.
In patients with a histologically proved primary malignancy, emergent radiation therapy to the spine is the most appropriate treatment, in most instances. Generally, the treatment is given in 10 to 15 fractions to a maximum dose of 2,000 to 3,000 cGy. The radiation ports usually encompass two levels above and below the area of epidural tumor. Most patients should continue to receive corticosteroids during the radiation therapy on a tapering schedule. Surgical intervention may be appropriate in patients without a tumor diagnosis, those who have received previous radiation to the spine, and those with radiationresistant tumors. Surgical procedures to remove epidural tumor are often extensive, requiring vertebral resection and spinal fusion. Not surprisingly, these aggressive procedures are often not appropriate for frail, elderly patients. Patients with recurrent or progressive epidural tumor in a previously radiated area may be candidates for a second course of radiation, if surgery is not feasible. In this instance, repeat radiation appears to carry a minimal risk of radiation myelopathy (55).
Prognosis
The presence of bony metastases implies advanced cancer, and most patients will die within 6 to 12 months of their systemic malignancy. The presence of epidural tumor will not usually hasten death unless the patient develops a complication of paralysis, such as deep venous thrombosis and pulmonary embolus, urosepsis from neurogenic bladder, or sepsis from decubitus ulcers. Timely diagnosis and treatment of epidural cord compression will reduce the likelihood that the patient will spend his or her remaining days wheelchair bound and dependent on others. If treatment is given before the development of severe neurologic dysfunction, the prognosis for neurologic recovery or maintenance of function is good. If treatment is not begun until after the patient is paraplegic and incontinent, then it is highly unlikely that steroids and radiation will bring recovery of function.
Only gold members can continue reading. Log In or Register to continue