HISTORY: Are the visual symptoms (1) monocular or binocular; (2) transient or permanent?; (3) What was the pattern of onset and were there (4) fluctuations or (5) associated symptoms (pain, diplopia, oscillopsia)?
AFFERENT EXAMINATION
(1) Acuity: Check each eye separately w/correction (>40 yo require near correction). Pinhole occlude (or paper w/pinhole) to exclude refractive error. (2) Color vision (color plates, red desaturation). (3) Pupillary response to light & near; compare size (differences in dark or light environment), symmetry, shape & look for APD (most detectable w/dim stimulus). (4) Visual fields, as w/other exam elements, each eye tested separately. (5) Funduscopy: Use dilating drops; if not possible, try small light at dimmest setting to ↓ glare; examine right eye (OD) w/your right eye & left eye (OS) w/your left eye; must be close to patient: color & quality of optic disc & neuroretinal rim, degree of cupping, arteries & veins, venous pulsations at edge of optic cup, quality of nerve fiber layer (NFL), peripapillary changes (hemorrhage, swelling, infiltrates), & macula.
EFFERENT EXAMINATION
Evaluate (1) ductions (eye mvmts of each eye independently) & (2) versions (eyes moving together), saccades (fast mvmt toward a target—are they full?; hypo or hypermetric?) & pursuits (following an object—was there any breakdown?), adventitious eye mvmts in primary & eccentric gaze, such as nystagmus, square wave jerks, nystagmoid movements, or opsoclonus. If strabismus (ocular misalignment) not apparent w/duction or version testing, do (3) alternating cover testing while pt fixates on target in primary, right-, left-, & upgaze as well as head tilts; w/mild left abducens palsy, for example, only sign may be a subtle esotropia on left gaze (by alternate cover testing). Observe is there is any (4) asymmetry with eyelids and orbits: ptosis, lid retraction, proptosis, tenderness on palpation, orbital bruit.
ANATOMY OF THE AFFERENT VISUAL PATHWAY
Retina: Photoreceptors (outer) → retinal ganglion cells (inner) → unmyelinated NFL (innermost retina); NFL axons travel to (and ‘form’) optic disc. Retinal projections: mainly lateral geniculate nucleus (LGN), also pretectal nucleus (pupillary light reflex pathway), superior colliculus (fixation, saccades, vergence, smooth pursuit), & hypothalamic suprachiasmatic nucleus (circadian rhythms). NFL axon paths: Foveal NFL → to optic disc (maculopapillary bundle); temporal retina NFL above & below fovea → disc in arced path (as arcuate bundles), respects horiz. meridian; nasal retina NFL axons → directly to disc. Arterial supply: Ophthalmic a. (ICA branch) travels w/ON in optic canal, branches into central retinal artery (travels in ON to supply inner retina) & long & short post. ciliary arteries (supply ON head, ciliary body, choroid, outer retina); 1/3 population have cilioretinal artery (from post ciliary circulation) to supply central macula. Venous drainage: Veins follow retinal & ophthalmic a., exiting orbit through sup & inf orbital fissures → cav. sinus & pterygoid plexus. Field defects: vascular dzs of temporal retinal NFL & optic disc & retinal arterial supply may produce field defects that respect horiz. meridian; primary retinal dzs do not. (prechiasmal dzs respect vertical meridian).
Optic nerve (ON): Site where retinal NFL axons converge. Axons become myelinated post. to lamina cribrosa (w/in anterior ON). Four portions: intraocular, intraorbital, intracancicular, intracranial. Blood supply: (1) anterior nerve & disc—post. ciliary arteries via ophthalmic artery; (2) post. nerve—pial circulation & central retinal/ophthalmic artery. Topographic representation of retina preserved in ON. ON exits orbit through optic canal (w/ophth. artery & oculosympathetics). Subarachnoid space surrounds ON (anterior limit is lamina cribrosa). Field defects 2/2 ON dz can be global or regional; divided by affected area: (1) temporal retina—horizontal altitudinal, arcuate, central, & centrocecal; (2) nasal retina—step-like; enlarged blind spots occur when optic disc swells, displaces and disturbs adjacent photoreceptors.
Optic chiasm (OC): Contains crossed fibers from nasal-& uncrossed fibers from temporal-retina. Located above pituitary/sella. Blood supply: Hypophyseal artery branches inferiorly (via ICA) & ACA branches superiorly. Fairly infarct resistant. Field defects: Categorized by affected area of OC: (1) central (crossing fibers)—inf, sup, or full bitemporal hemianopia (field defect begins near vertical midline, not peripherally); (2) anterior chiasm—junctional scotomas: ON-type defect (e.g., central scotomas) in one eye & chiasm-type defect (e.g., superotemporal defect) in the other.
Optic tract: Fibers from c/l nasal-& i/l temporal-retina. Blood supply: Ant choroidal a. (via ICA) & PComm. Lesion → c/l incongruous homonymous hemianopia (w/o central sparing).
LGN: 6-Layered thalamic nucleus; gets input from optic tract. Blood supply: Ant choroidal artery (ICA branch) → med & lat LGN; post. choroidal artery (PCA branch) → hilum of LGN. Field defects (in stroke): c/l incongruous hemianopia (entire LGN), sectoranopia (lateral choroidal, PCA branch), reverse sectoranopia (anterior choroidal, ICA branch).
Optic radiations: Post-LGN tracts divided superiorly (occipitoparietal) & inferiorly (occipitotemporal; Meyer loop). Blood supply: Anterior radiations via ant. choroidal & MCA; superior radiations via superior MCA; inf & postradiations via MCA & PCA. Field defects: c/l congruent homonymous hemianopias; inferior division lesion: c/l superior homonymous hemianopia (“pie in the sky”); superior division: c/l inferior homonymous hemianopia.
Primary visual cortex (striate cortex): Target of optic radiations; site of synapses from LGN. Blood supply: mainly PCA, but occipital pole also PCA contributions. Lesions → c/l congruent homon. hemianopia; ant. mesial OL lesion can produce c/l monocular peripheral crescent-shaped field defect. Macula represented at occipital pole → lesions ant. to pole spare macular vision.
Visual association cortex:“Where” visual stream is superior (OL/PL). Lesions → visuospatial deficits (e.g., Balint syndrome, visual attention, spatial organization). “What” visual stream is inferior (OL/TL). Lesions → semantic deficits (e.g., prosopagnosia, object recognition, color). Blood supply: OL/PL regions via superior MCA branches; OL/TL regions via PCA & inferior MCA branches.
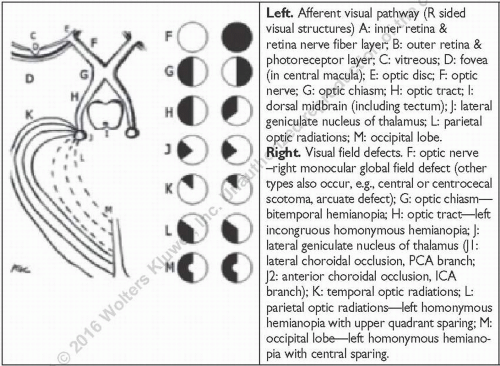
Left. Afferent visual pathway (R sided visual structures) A: inner retina & retina nerve fiber layer; B: outer retina & photoreceptor layer; C: vitreous; D: fovea (in central macula); E: optic disc; F: optic nerve; G: optic chiasm; H: optic tract; I: dorsal midbrain (including tectum); J: lateral geniculate nucleus of thalamus; L: parietal optic radiations; M: occipital lobe. Right. Visual field defects. F: optic nerve – right monocular global field defect (other types also occur, e.g., central or centrocecal scotoma, arcuate defect); G: optic chiasm—bitemporal hemianopia; H: optic tract—left incongruous homonymous hemianopia; J: lateral geniculate nucleus of thalamus (J1: lateral choroidal occlusion, PCA branch; J2: anterior choroidal occlusion, ICA branch); K: temporal optic radiations; L: parietal optic radiations—left homonymous hemianopia with upper quadrant sparing; M: occipital lobe—left homonymous hemianopia with central sparing.
TRANSIENT MONOCULAR VISUAL LOSS
Def: Can be ischemic (amaurosis fugax) or non-ischemic. Pt’s perception of monocular might be misleading (e.g., pts often localize homonymous hemianopia to the eye of the temporal field deficit). Epid: Ischemic transient monocular visual loss (TMVL) usu in elderly.
P/w: (1)Ischemic: Usu painless, acute-onset & brief (sec-min); often horizontal altitudinal; w/common carotid or ICA atheroembolism or less frequently severe carotid stenosis causing retinal or choroidal hypoperfusion, ±other lateralizing TIA symptoms (transient language changes, c/l wkness/numbness); GCA usually elderly, with jaw claudication and temporal tenderness, ± PMR. (2) Nonischemic: Unlike ischemic, sx may be more vague; wide DDx, but common/notable dxs: blurring, ↓ w/blinking/artificial tears → dry eyes; “positive” visual sx (flashing lights) → migraine; visual obscurations w/bending forward → optic disc swelling; Uhthoff phenomenon (old demyelination); eye pain → angle-closure glaucoma; ↓vision w/eye mvmts→ orbital tumor; HA; APD (retinal artery vasospasm, demyelination, often migraine).
DDx: (1) Ischemic TMVL: Ophthalmic, central or branch retinal, or posterior ciliary artery dz. ICA atheroembolization/in-situ thrombus of ophthalmic, central retinal or branch retinal arteries (can be 2/2 GCA) or veins (i.e., impending CRVO/BRVO). Posterior ciliary a. thrombosis or inflammation/vasculitis via impending anterior ischemic optic neuropathy (AION) (can be 2/2 GCA, which is a treatable vascular emergency). (2) Nonischemic TMVL: Dry eyes, angle-closure glaucoma, anterior segment dz (e.g., dry eyes, hyphema), retinal detachment, ON compression (orbital tumor), optic disc swelling including papilledema & drusen, migraine (may evolve into ischemic TMVL).
Dx: (1) Obtain prior ophth. hx & vascular risk factors (including carotid & cardiac dz). (2) Eye exam: Nonischemic TMVL: Routine eye exam (r/o anterior segment dz & ↑intraocular pressure). Ischemic TMVL, may see refractile emboli w/in retinal arteries on funduscopy (Hollenhorst plaques). (3) Eval for GCA (ophthalmologic emergency) via CBC, ESR, & CRP (none has good specificity). (4) Vessel imaging from aortic arch to ophthalmic arteries (e.g., head & neck CTA or MRA, or ultrasound); carotid bifurcation of special interest for atheroembolic dz. (5) Cardiac ultrasound (ejection fraction, valves, presence of PFO, r/o thrombus). (6) Consider hypercoagulable panel in pts w/o vascular risk factors & nl vessels. (7) Consider fluorescein angiogram: delayed choroidal filling suggests GCA; sluggish venous flow suggests impending CRVO/BRVO.
Rx: Ischemic TMVL: Secondary stroke prevention w/risk factor modification; CEA if due to symptomatic ICA stenosis. Nonischemic TMVL: Ophthalmologic or neurologic care based on etiology.
Prognosis: In cases of ICA atheroembolism-related TMVL, 25% chance of stroke over 3 yr in significant carotid stenosis; 4% annual risk of death (NEJM 2001;345:1084; Neuro Clin 2010;28:619).
RETINAL AND OPTIC NERVE ISCHEMIA
CRAO and BRAO: Vascular urgency since cerebral infarction may ensue. Central retinal and branch retinal artery occlusions ≥ acute monocular visual loss, usually painless. Permanent loss, but might be preceded by one or more (stuttering) episodes of TMVL or cerebral TIA. Since ocular vascular supply is through ICA branches, ocular ischemic symptoms can be secondary to distal (ophthalmic artery) or proximal (cardiac) processes. If ICA severe stenosis/occlusion ≥ retinal blood supply may be from ECA, and steal retrograde flow from eye (ophthalmic a.) to brain. P/w: CRAO: acute, monocular, severe visual loss (may be far peripheral visual field sparing); RAPD common; fundus w/attenuated retinal arteries, sometimes emboli can be visualized, retinal edema (whitening) after a few hours from retinal thickening/lost of transparency & cherry red spot (at fovea, where retina is most thin and red choroid still visible); BRAO: acute, monocular, partial visual loss; variable RAPD; fundus w/altitudinal (superior or inferior) retinal thickening/whitening w/corresponding field defect (superior BRAO causes inferior visual field defect).
Ophthalmic artery occlusion: similarly to CRAO; ICA large emboli vs. in-situ thrombosis/plaque. DDx: retinal vein occlusion (subacute over days). Dx: Similar to cerebral ischemia work up; exclude GCA in pts >50 yo and other GCA risk factors. Association of BRAO/CRAO + AION highly suggestive of GCA; recurrent BRAO is part of Susac syndrome (rare vasculopathy of small retinal, cochlear and cerebral arteries). Rx: No clear treatments. IA thrombolysis (catheterization of ophthalmic artery) or IV tPA with limited evidence of benefit. Focus on prevention of subsequent vascular events. Pts admitted for secondary stroke prevention (Am J Ophthalmol 2014;157(6):1119).
Optic Nerve ischemia—Def: ↓ blood supply to any portion of ON— short posterior ciliary arteries to ON head w/anterior ON ischemia & long posterior ciliary arteries (from ophthalmic artery) and pial vasculature w/posterior ON ischemia. Classified based on (1) location: AION, anterior optic dz; posterior ischemic optic neuropathy (PION), posterior or retrobulbar (i.e., behind lamina cribosa) ON. (2) Underlying cause: “arteritic” or “non-arteritic.” “Arteritic” synonymous w/GCA-related ischemia. Emboli not believed to obstruct posterior ciliary arteries.
Epid: AION much more common (90%). (1)Nonarteritic AION (NA-AION): Typically >50 yo (but can occur at any age). A/w small optic cups (cup-to-disc ratio < 0.3), hypotension, anemia, cardiac or spinal surgeries, hypercoagulable disorders, acute ↑ intraocular pressure, radiation. Controversial risk factors: vascular risk factors/dz, amiodarone, sildenafil; since dz of small vessels, not related to ipsilateral ICA stenosis or emboli; rare cases 2/2 ON head drusen or papilledema (from “vascular crowding”). (2) Arteritic AION (A-AION): Age >50 yo, a/w GCA; often +PMR. (3) PION: Typically in setting of severe blood loss (cardiac or lengthy spine surgery in prone position) or prolonged ↓ BP; pts >50 yo; rarely from GCA or fungal infxn (e.g., mucor).
P/w: Disc edema present in AION. (1)NA-AION: Acute monocular vision (mild to severe); worst at onset, but nadir may take days (to weeks); pt may notice inferior field defect; rarely binocular or sequential unless GCA-related; usu painless (but mild pain may be reported). (2)A-AION: as w/NA-AION, but often w/prodromal TMVL; ±sx of GCA & PMR: Jaw claudication, HA, head tenderness, malaise, wt loss, fevers, sweats, hip, & shoulder aches. (3)PION: Rapid-onset or awakes from surgery w/severe binocular (or monocular) visual loss; optic discs show pallor 4-6 wks after event.
Dx: (1) Si/sx of optic neuropathy—↓ acuity, dyschromatopsia, APD, edematous hyperemic optic disc (pallor w/edema in A-AION), inf. altitudinal field defect common (but can be superior or global); disc pallor chronically. (2) w/NA-AION, other eye w/small cup-to-disc ratio (<0.3). (3) Palpate for nodular, thickened, pulseless, & firm temporal arteries for GCA eval. (4) CRP, ESR, & CBC (anemia & thrombocytosis in GCA). (5) Temporal artery bx; b/l bx ↑’s sensitivity (6) ±brain & orbital MRI w/gado: eval ONs; typically nl in acute phase; may show DWI/ADC abnlities in PION; chronically ↑ T2 signal of ON in AION & PION (also helps r/o other causes of optic neuropathy).
DDx: Optic neuritis—F > M, younger pts, pain w/eye mvmts, a/w MS; tends to improve. ON infiltrative/infectious/compressive lesions; slower course if neoplastic-related.
Rx:NA-AION: no proven Rx. A-AION: Immediate IV methylprednisolone (250 mg every 6 h for 3-5 days), then PO prednisone (1 mg/kg/d) to protect fellow eye; rx started immediately on presumed dx (don’t wait for ESR or temporal artery bx). PION: No proven Rx; A-AION Rx regimen if GCA suspected.
Prognosis:NA-AION: Affected eye recurrence <5%; other eye ˜15% at 5 yr; poor visual recovery. A-AION: Progressive visual loss of involved eye; visual loss of fellow eye in ˜40% if untreated; risk of MI & stroke; can recur if steroids are tapered too quickly; recurrences yr after rx are exceedingly rare; poor visual recovery. PION: Poor visual recovery.
A-AION
NA-AION
Optic Neuritis
Age
>50
Typically >40
Typically 20s-30s
Pain
HA, jaw claudication
Usu not
Yes, w/eye mvmts
Dx
HPI/exam, ESR/CRP, TA bx
HPI/exam
HPI/exam
Pathogenesis
Vasculitic
?Ischemic
Immune-mediated
↓ acuity, APD, dyschromatopsia
Yes
Yes
Yes
Disc edema
Yes (±pallid edema)
Yes (may be sectorial)
Only 1/3 of pts
Disc hemorrhages
Yes
Yes
No
Optic cup of fellow eye
Nl
Small
Nl
Visual field defect
Any ON type defect
Altitudinal or arcuate, typically inferiorly
Any ON-type defect; central/arcuate defects common
Rx
Steroids w/slow taper
Risk factor modification
Consider IV steroids
Prognosis
Severe visual loss; risk of further/fellow eye visual loss w/o Rx
Variable visual loss, static; <5% recurrences same eye, but 15% fellow eye involvement in 5 yr
Most recover; risk of developing MS
OPTIC NEURITIS & DEMYELINATING OPTIC NEUROPATHIES
See Optic Neuritis section in Multiple Sclerosis and Other CNS Inflammatory Demyelinating Diseases chapter.
HEREDITARY, TOXIC, & METABOLIC OPTIC NEUROPATHIES
Def: Various ON dzs, most often affect central vision (via maculopapillary bundle).
P/w: Insidious, usually painless, bilateral and symmetric central visual loss (unless otherwise noted).
Dx: Exam: Symmetric, ↓acuity, dyschromatopsia, central visual field defects, disc pallor.
Imaging: Brain & orbital MRI w/gado to exclude compressive lesions.
Specific causes
B12 deficiency-related optic neuropathy: Def: Malnutrition-related demyelination of ON stemming from maculopapillary bundle; vision loss may precede anemia and other neurological sx. Epid: Pernicious anemia (most common in developed countries), enteritis or small intestine resection, veganism. DDx: DOA, chiasmal lesion (occasional bitemporal field defects). Dx: Optic pallor, centrocecal field defects, memory dysfxn, ↓ vibratory & position sensation, macrocytic anemia, ↓ B12 & ↑ homocysteine/methylmalonic acid, brain MRI w/white matter dz. Rx: IM hydroxycobalamin. Prog: Visual stability w/Rx; variable improvement.
Thiamine deficiency: Rare; vitamin B1 is cofactor for several mitochondrial enzymes. ON may occur w/Wernicke encephalopathy (alcohol abuse, malnutrition). P/w: acute/subacute visual loss, disc swelling. Dx: serum thiamine has low Se and Sp, so supplementation should be done empirically. Prog: complete recovery.
Methanol-related optic neuropathy: Def: Toxin-mediated white matter dysfxn. P/w: Lethargic; HA; vomiting abdominal pain; blindness. Epid: Homemade ETOH, methanol-containing industrial products. Dx: Disc swelling; metabolic acidosis; brain MRI w/putamen hemorrhage and infarct. Rx: Ethanol or fomepizole IV, bicarbonate IV. Prog: Poor visual recovery.
Tobacco-alcohol amblyopia: Def: Presumed additive malnutrition & toxin-mediated optic neuropathy; past epidemics in Cuba & Jamaica in association w/cigar smoking & cassava, resp. Epid: Smoking, excessive ETOH intake, malnourished. Ddx: B12 deficiency-related optic neuropathy, dominant optic atrophy, compressive optic neuropathies. Dx: Possible peripapillary hemorrhage in early stages; check B12 levels. Rx: IM hydroxycobalamin, multivitamins, smoking, & ETOH cessation. Prog: Visual stability w/Rx; variable improvement.
Linezolid: antibiotic designed for MRSA and VRE, disrupts protein synthesis in mitochondria. Dose dependent optic and peripheral neuropathy. Dx: clinical. Rx: discontinuation. Prog: some recover from ON, peripheral neuropathy usually permanent.
Cyclosporine and Tacrolimus: immunosuppressants used to prevent rejection after organ transplant. Both cause PRES and more rarely, optic neuropathy. Likely 2/2 elevated ICP and papilledema. Case reports w/o improvement after discontinuing drug, but visual loss stabilized.
Leber hereditary optic neuropathy (LHON): mitochondrial DNA mutation, affects mostly men 15-35 yo; +/- maternal Fhx. Painless subacute visual loss in one eye, followed by contralateral eye in weeks to months; final acuity 20/200 OU. Dx: visual fields with central and cecocentral deficits; lack of leakage on retinal angiography (pseudoedema); genetic test. No proven rx.
Radiation optic neuropathy (J Neuro-ophth 2004;24:243): Def: Radiation-induced dz of ON. P/w: Acute/subacute > chronic visual loss yrs after exposure; (typically 2 yr); monocular or binocular; may be sequential visual loss. Epid: Prior radiation exposure of at least 50 Gy. Dx: Exam w/retrobulbar optic neuropathy or retinopathy, more common in pts with underlying vascular dz; pallor chronically; brain & orbital MRI w/gado shows enhancement & enlargement of involved region. Ddx: Tumor. Rx: None of proven efficacy; may try hyperbaric oxygen, corticosteroids. Prog: Poor visual outcome; may affect any portion of visual pathway (chiasm, tract, radiations).
Other etiologies: Ethambutol, ?sildenafil, other organic solvents (toluene).
May confirm presence of pathologic disc swelling (showing disc leakage of dye); may help delineate extra-disc dz (i.e., retinal dz)
INFLAMMATORY-INFILTRATIVE OPTIC NEUROPATHIES
Sarcoid-associated optic neuropathy (Sem Ophth 2008;23:157): Def: Granulomatous inflammation in ON or chiasm. P/w: Typically subacute, severe monocular visual loss (variable pain); co-existent diabetes insipidus (especially if chiasm involved), HAs (meningitis), facial nerve palsies; often preceded by systemic sarcoidosis (pulmonary, skin); other ocular manifestations are more common (uveitis, retinal vasculitis). Epid: Age 20-40; African descent. Dx: Disc granulomas & swelling (if anterior dz); orbital & brain MRI w/gado (enhancement & enlargement of ON or chiasm, meningeal enhancement, pituitary-hypothalamic involvement); chest CT; serum ACE; ↑ protein & WBC (mild) in CSF; “tissue is the issue” biopsy of skin, lacrimal glands, lymph nodes, lung, or brain. Ddx: Optic neuritis, optic perineuritis, primary neoplastic or metastatic optic neuropathy. Rx: Initial high-dose corticosteroids, chronic maintenance steroids; Chronic Rx: Consider methotrexate, anti-TNF-α gents, cyclophosphamide. Prog: Typically relapsing-remitting course, vision may be restored w/Rx.
Lupus-associated optic neuropathy (Autoimmune Dis 2012;290898): Def: Myriad ocular manifestations due to many mechanisms—vasc. occlusion, inflammation, demyelination of ON. P/w: Subacute or chronic monoc. or binoc. visual loss (variable pain); co-existent spinal cord dz; often preceded by SLE (skin, joint, kidney, serous linings), but may be first sign; rare pseudotumor cerebri-like presentation. Epid: 20-30s, F >> M. Dx: Fundus often wnl; disc pallor if chronic; orbital & brain MRI w/gado (variable ON enhancement, WM dz); serum ANA (sens), anti-dsDNA, and anti-Smith (higher spec), antiphospholipid syndrome (APS) abs. Rx: Initial corticosteroids, consider other agents (methotrexate, azathioprine, cyclophosphamide, plasmapheresis, IVIg, anticoagulation in APS). Prog: Chronic or relapsing-remitting course; visual improvement may be seen, earlier steroids are associated w/better prognosis.
Other autoimmune-related optic neuropathies (very rare)
Optic perineuritis—subacute monocular visual loss (variable pain); disc edema & retinal hemorrhages, ON sheath enhancement on MRI. Ddx: Sarcoidosis, TB, syphilis, & Lyme dz. Rx: Treat underlying dz or w/corticosteroids if idiopathic.
Sjögren-related optic neuropathy—Optic neuritis-like presentation w/acute or subacute painful monocular visual loss; systemic (xerostomia, arthralgia, myalgias) & ocular (keratoconjunctivitis) signs, variable WM dz on MRI; Dx: rheumatoid factor (50% pts), Ro and La. Rx: Consider corticosteroids and immunosuppressive therapy.
Behcet dz-related optic neuropathy—Visual loss can occur from optic neuritis, neuroretinitis, or↑ ICP w/papilledema; retinal vasculitis affecting veins, and anterior chamber inflammation; systemic si/sx of Behcet’s (genital & oral ulcers, lymphadenopathy). Rx: Immunomodulatory (& acetazolamide if ICP culprit).
Chronic relapsing inflammatory optic neuropathy (CRION) (Brain 2003;126:276-284)—Recurrent, acute/subacute painful visual loss (i.e., recurrent optic neuritis). Vision loss may manifest during steroid taper. Unclear pathogenesis, but elevated ANA (79%) and anticardiolipin are common (82%) (Am J Ophthalmol 1982;94:11).
INFECTIOUS OPTIC NEUROPATHIES
Lyme-related optic neuropathy (J Neuro-ophth 1997;17:108): Def: ON dysfn 2/2 Borrelia. Subdivided based on mechanism: (1) Intracranial HTN (papilledema); (2) post- or parainfectious demyelination of anterior ON (papillitis); (3) Direct infxn of ON & retina (neuroretinitis). Role of (2) & (3) in Lyme dz is controversial. Lymerelated information below further based on these subdivisions (1, 2, & 3).
Only gold members can continue reading. Log In or Register to continue