Neuroanatomy
CEREBRAL CORTEX
There are many large textbooks with extensive writings and illustrations providing all the known specifics about the anatomy of the nervous system. If you are looking for that sort of detail, then you are reading the wrong book. We—on the other hand—have tried to limit our discussion of neuroanatomy to those structures frequently identified in the scientific articles that are relevant to the clinician treating mental illness. First, we feel compelled to review a bit about the developing brain. You can best understand how the brain anatomy is organized by remembering how it formed itself in the first place.
Development
The fertilized egg quickly divides and differentiates into an embryo with three cell lines: the endoderm, mesoderm, and ectoderm. A portion of the ectoderm folds and forms the neural tube that becomes the rudimentary nervous system. The most anterior cells of the nervous system spend the ensuing weeks proliferating, migrating, and developing into the different regions of the brain.
The process of differentiating is almost unbelievable. How one undeveloped cell decides it should be a neuron while a similar one becomes an astrocyte is simply amazing. The evidence suggests that chemical signals between cells turn the DNA on and off, which then controls the destiny, but orchestrating all this is almost beyond comprehension.
The migration of cells to their appropriate location in the brain is another remarkable aspect of the developing brain. Neuroblasts (undeveloped neural cells) multiply in an area called the ventricular zone. Then they shinny up radial cells (specialized glial cells) that form a kind of scaffolding to build the cerebral cortex (Figure 2.1). As the neuroblasts reach the surface of the brain, they differentiate into the various mature neurons and astrocytes that make up the gray matter.
Other neuroblasts migrate tangentially from the bottom of the ventricles. These neuroblasts typically develop into the inhibitory interneurons. They start in a different location and must come up and around before they intermingle with the other neuroblasts climbing the radial cells. It boggles the mind that all these cells find their correct location and make the right connections while we can barely find what we are looking for in Walmart.
A residual portion of the ventricular zone remains in the adult brain and allows limited neurogenesis to continue beyond the fetal stage (Figure 8.3)—more on this topic in Chapter 8.
The migrating and differentiating neuroblasts slowly form into the six layers of the cerebral cortex. Figure 2.2 shows how the process proceeds. The inner layers are formed first: layer IV, then layer V, and so on. This means that cells destined for the outer layers must climb past the other neurons before locating their place in the brain.
DISORDER
MENTAL RETARDATION
The migration of neurons to their specific location is a critical and venerable period of brain development. Fetal alcohol syndrome may in part be a result of aberrant migration due to the toxic effects of ethanol. Radiation is another insult that deters the traveling neuron. Studies of pregnant Japanese women who were in proximity to the epicenter when the atomic bombs were dropped found that 80% of the children who developed severe mental retardation were exposed to radiation between 8 and 16 weeks after conception— the time of peak migration.
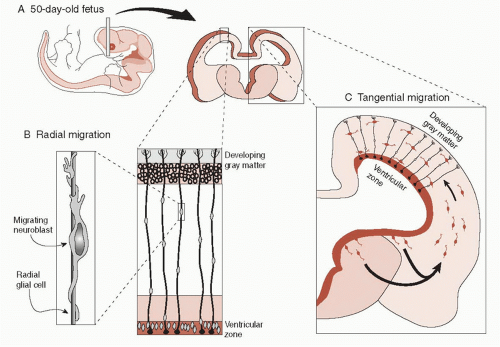 FIGURE 2.1 • A. Cross section of the brain of a 50-day-old fetus. b. Neuroblasts climb up the radial glial cells to the developing gray matter. C. Inhibitory neurons develop from neuroblasts that migrate tangentially from lower regions of the brain. |
The cerebral cortex is made up of white matter and gray matter (Figure 2.3). The gray matter is where the nerve cells and synapses reside. This is where the action occurs psychologically—where we think and feel—where depression, schizophrenia, and dementia likely develop. The white matter is primarily myelinated axons transporting impulses between the gray matter and lower brain structures. The white matter makes up the circuits that connect the regions of the brain—connecting cabling.
When we say a “neuron,” we are usually thinking of the large pyramidal neurons with their triangularshaped cell bodies. They make up approximately 75% of the cortical neurons. They have a single apical dendrite pointed toward the pial surface and a number of basilar dendrite branches projecting horizontally. The axons project (and send impulses) to other cortical regions or the deeper structures of the subcortex.
The pyramidal neurons receive signals from the other brain regions as well as from the local interneurons. The afferent signals from other regions are typically excitatory signals that encourage the neuron to generate its own impulse. The interneurons are typically γ-aminobutyric acid (GABA) neurons, which inhibit the pyramidal neuron and reduce the likelihood it will fire.
Brodmann’s Areas
In the early part of the 20th century, many neuroanatomists were struggling to divide the neocortex into structurally distinct regions. Korbinian Brodmann, a German neurologist, was working in a psychiatric clinic where he was influenced by Alois Alzheimer to pursue a career in neuroscience basic research. After extensive analysis of the human and monkey neocortex, he published in 1909 his classic work Comparative Localization Studies in the Brain Cortex, Its Fundamentals Represented on the Basis of Its Cellular Architecture.
He had divided the neocortex into 52 regions based on the size, number, and density of the cells as well as the local connections and long tract projects to and from the subcortical regions (Figure 2.4). Brodmann’s scheme is still widely used and often mentioned in the scientific literature.
He had divided the neocortex into 52 regions based on the size, number, and density of the cells as well as the local connections and long tract projects to and from the subcortical regions (Figure 2.4). Brodmann’s scheme is still widely used and often mentioned in the scientific literature.
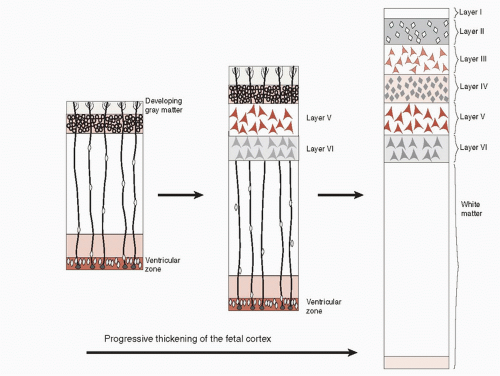 FIGURE 2.2 • The six layers of the cerebral cortex develop in reverse order as the neuroblasts migrate up from the ventricular zone. (Adapted from Bear MF, Connors BW, Paradiso MA, eds. Neuroscience: Exploring the Brain. 3rd ed. Baltimore, MD: Lippincott Williams & Wilkins; 2007.) |
prefrontal Cortex
Everybody loves the prefrontal cortex (PFC). It is one of the anatomic structures that distinguishes humans from other mammals. Technically, it is the cortex in front of the motor cortex. Brodmann calculated that the PFC as a percentage of the total cortex is 3.5% in the cat, 7% in the dog, 8.5% in the lemur, 11.5% in the macaque, 17% in the chimpanzee, and 29% in humans (Figure 16.10). Dysfunction in the PFC is implicated as a possible source of pathology in many psychiatric disorders— depression, schizophrenia, anxiety, and attention-deficit/hyperactivity disorder (ADHD), as well as disorders of anger and violence.
There are four regions of the PFC that are frequently mentioned in the scientific literature (Figure 2.5): dorsolateral PFC, anterior cingulate gyrus, ventromedial PFC, and orbital PFC. Unfortunately, there is no consensus on the wording of these regions. Different terms are often combined to describe an area of interest, for example, ventrolateral and medial orbital. The ever-expanding jargon of the scientific writers is one of the great challenges of understanding neuroscience.
Neurologists, assessing and following up patients with injuries (e.g., Phineas Gage—see Figure 11.4), have identified three different
syndromes associated with frontal lobe damage. The location, core characteristics, and common symptoms are briefly outlined in Table 2.1. The three syndromes roughly correlate with the three regions of the PFC. Although it is appealing to associate a location with specific behavioral pattern, it is not that simple. Most patients have clinical features of more than one of the syndromes because few lesions are confined to one region. Furthermore, recent imaging studies do not always find correlations between the anatomy and the traditional syndromes.
syndromes associated with frontal lobe damage. The location, core characteristics, and common symptoms are briefly outlined in Table 2.1. The three syndromes roughly correlate with the three regions of the PFC. Although it is appealing to associate a location with specific behavioral pattern, it is not that simple. Most patients have clinical features of more than one of the syndromes because few lesions are confined to one region. Furthermore, recent imaging studies do not always find correlations between the anatomy and the traditional syndromes.
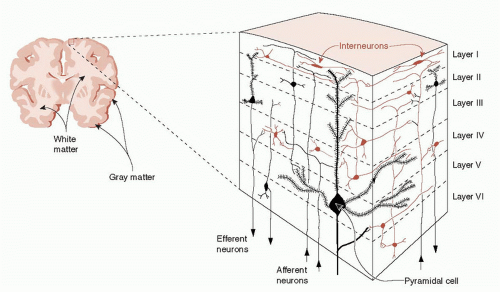 FIGURE 2.3 • The six layers of the neocortex, from the pial surface above layer 1 to the white matter below layer 6. (Snell RS. Clinical Neuroanatomy: A Illustrated Review with Questions and Explanations. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.) |
TABLE 2.1 The Three Traditional Frontal Lobe Syndromes and the Associated Regions and Symptoms | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


