(1)
Department of Neurosurgery, Radboud University Nijmegen Medical Center, Nijmegen, The Netherlands
Abstract
Neuroendoscopic surgery has evolved from an initially diagnostic modality over a treatment modality for obstructive hydrocephalus to a widespread neurosurgical technique. It reflects the tendency of modern neurosurgery to aim towards minimum invasiveness. Transventricular neuroendoscopic approaches allow the treatment of several pathologies inside the ventricular system, such as obstructive hydrocephalus and intra- and paraventricular tumors and cysts. Skull base transnasal transsphenoidal endoscopy is increasingly used to resect large skull base lesions (pituitary adenomas, craniopharyngiomas, meningiomas, and clival chordomas). An endoscope may be used to assist microneurosurgery in virtually any kind of neurosurgical procedures, particularly in aneurysm and tumor surgery.
Several endoscopes have been developed in the last 20 years, with brilliant visualization and illumination, high-quality equipment for intricate surgical manipulations, small outer diameter, and an ergonomic and convenient way of handling the endoscope and the instruments in order to compete with minimally invasive microneurosurgery to cover the needs of different surgical procedures. Mechanical and pneumatic fixation holding devices have been developed to enable stabilization of the endoscope for lengthy procedures. Significant progress has been achieved in the design of light sources and cameras. Modern three-chip technology provides impressive color depth and brilliant red differentiation. The latest Full HD technology delivers lag-free images, even with rapid camera movements.
When we learn and understand more various CNS pathologies, the targets and demands for endoscopic procedures will change accordingly. Telemanipulated neurosurgery, with supervisory-controlled robotic systems, or shared control systems or even fully robotic telesurgery as well as the development in nanotechnology will be needed to address future indications for minimally or even ultramicro-access neurosurgery.
7.1 Introduction
Neuroendoscopic surgery has evolved from an initially diagnostic modality over a treatment modality for obstructive hydrocephalus to a widespread neurosurgical technique. It reflects the tendency of modern neurosurgery to aim towards minimum invasiveness, that is, access and visualization through the narrowest practical surgical approach with, at the same time, maximum effectiveness. Transventricular neuroendoscopic approaches allow the treatment of several pathologies inside the ventricular system, such as obstructive hydrocephalus and intra- and paraventricular tumors and cysts.
However, an endoscope may be used to assist microneurosurgery in virtually any kind of neurosurgical procedures, particularly in aneurysm and tumor surgery. This endoscope-assisted microneurosurgery allows precise clipping of aneurysms and visual control to avoid inadvertent clipping of perforators and parent arteries and allows to “look around the corner” in tumor surgery to identify vital structures that are hidden behind the tumor itself or bony protrusions. Endoscope-controlled microneurosurgery is the replacement of the operating microscope by a larger lenscope. It is best illustrated by the rapidly evolving technique of endoscopic endonasal transphenoidal surgery that allows the treatment of pathologies of the sellar and parasellar region and frontal skull base such as pituitary adenomas, craniopharyngiomas, meningiomas, and clival chordomas, with the advantage of a wide vision of the surgical field.
This evolution occurred in response to the reported benefits of endoscopic surgery compared to conventional surgical procedures for patients. The use of neuroendoscopic surgery has increased exponentially during the past 10 years. Previously lengthy and difficult procedures now are being performed endoscopically. Advances in instrumentation, dissection and hemostasis techniques, and improved camera technologies have simplified these procedures and expanded the application of the minimally invasive neurosurgical approach.
The earliest reported endoscopic neurosurgery was performed in 1910 when two children were treated for hydrocephalus by endoscopic fulguration of the choroid plexus. By 1960, technological advances in flexible and rigid lens endoscopes allowed for additional endoscopic procedures, but it was not rapidly adopted by neurosurgeons. In the 1970s it was Fukushima (Japan) who used fiber optics to inspect the ventricular system. Vries and Jones used it for the treatment of hydrocephalus and Prott and Oppel for the inspection of the subarachnoid space.
Further use of neuroendoscopy was hampered by the lack of dedicated endoscopes and dedicated instruments for the specific needs inside the ventricular system and subarachnoid space. When I started to use neuroendoscopy I used pediatric cystoscopes and flexible bronchoscopes and makeshift instruments to perform fenestrations and biopsies. But soon the development of such suitable and specially designed neuroendoscopic equipment started.
7.2 Neuroendoscopes and Endoscopic Equipment
Requirements for modern endoscopes suitable for neurosurgery are brilliant visualization and illumination, high-quality equipment for intricate surgical manipulations, small outer diameter of the endoscope, and an ergonomic and convenient way of handling the endoscope and the instruments in order to compete with minimally invasive microneurosurgery.
In 1986 Jacques Caemaert, from the Department of Neurosurgery of the University Hospital of Ghent, Belgium, designed the first prototype of a new multipurpose neuroendoscope. The requirements for this instrument were a maximum outer diameter of 6 mm, round in cross section to permit rotation around its own axis, a long rigid sheath suitable for freehand introduction with any stereotactic frame, simultaneous visual control and operating possibilities, and continuous irrigation via separate inlet and outlet channels which are themselves wide enough to take small auxiliary operating instruments. He developed this endoscope together with the company Richard Wolf, Germany, and is still in production in an updated form (Fig. 7.1).

Fig. 7.1
Wolf rigid neuroendoscope, with 6-mm outer diameter, three working channels, and sheath of 25 cm, long enough to be used in conjunction with the Leksell stereotactic frame, designed by Prof J. Caemaert, originally introduced in 1986, and still in production in an updated form (Richard Wolf GmbH, Knittlingen, Germany) (Photograph courtesy of Dr S. Sgouros)
Professor Michael Gaab, an endoscopic pioneer from Germany, developed an endoscopic system for intraventricular use in the early 1990s together with company Storz. It consists of a 6.5-mm rigid shaft, which is equipped with three channels for instruments, suction, and irrigation (Fig. 7.2). There are the so-called diagnostic optics that are larger than the therapeutic optics. When the latter is used, it fills up less space inside the shaft and leaves more room for instruments. The same company offers a variety of specific neuroendoscopic systems, e.g., the LOTTA neuroendoscope for intraventricular use designed by Professor Henry Schroeder (Fig. 7.3), the universal endoscopy set designed by Professor Philippe Decq, the Oi HandyPro system designed by Professor Shizuo Oi for pediatric patients (Fig. 7.4), and the endonasal transphenoidal endoscope set with Thumfart suction and irrigation system designed by Professor Martin Bettag and Peter Schäfer (Fig. 7.5). Each of these endoscope systems comes with a complete set of optics of different viewing angles (0° and 30°) and a multitude of purpose-designed instruments.




Fig. 7.2
Endoscope system Storz Gaab (Karl Storz GmbH & Co KG, Tuttlingen, Germany) (Photograph courtesy of Dr S. Sgouros)
Fig. 7.3
Endoscope system Storz Schroeder LOTTA, with main endoscope shaft, obturator, and optical rod lens. Some instruments (grabbing forceps and scissors) are shown as well (Karl Storz GmbH & Co KG, Tuttlingen, Germany) (Photograph courtesy of Dr S. Sgouros)
Fig. 7.4
Endoscope system Storz Oi Handy Pro, designed mainly for pediatric work, shown with its instrument set (grabbing forceps and scissors) (Karl Storz GmbH & Co KG, Tuttlingen, Germany) (Photograph courtesy of Dr S. Sgouros)
Fig. 7.5
Endoscope system Storz Bettag Schäfer with the Thumfart suction-irrigation system, specifically designed for transnasal skull base work (Karl Storz GmbH & Co KG, Tuttlingen, Germany) (Photograph courtesy of Dr S. Sgouros)
Another important company in this field, also from Germany, B. Braun/Aesculap, has developed in close cooperation with Professor Axel Perneczky from the University Hospital in Mainz, Germany, until his untimely death in 2009, several specialized endoscopic instruments and endoscopes. This led to the development of a modular system for all applications of endoscopic neurosurgery, called the MINOP® Modular Neuroendoscopy System.
The MINOP® system is a multifunctional and modular neuroendoscopy system for intraventricular indications and endoscope-assisted neurosurgery. It consists of three trocars, with outer diameters 3.2 mm/4.6 mm/6 mm, for diagnostic and therapeutic purposes; several instruments; electrodes; accessories; and especially two FULL HD compatible endoscopes, outer diameter 2.7 mm, viewing direction 0° and 30°. Its angled design makes the MINOP® system easy to handle and universal in use (Fig. 7.6). It has blunt distal tip of trocar and depth marking for atraumatic insertion and straight working channel for rigid instruments which increases control and precision. Its rigid instruments have steering wheel, which allows rotation of their tip without turning your holding hand and offers the possibility to work bi-instrumental with both hands. It has lateral connection of cables for unhindered view along the trocar shaft.
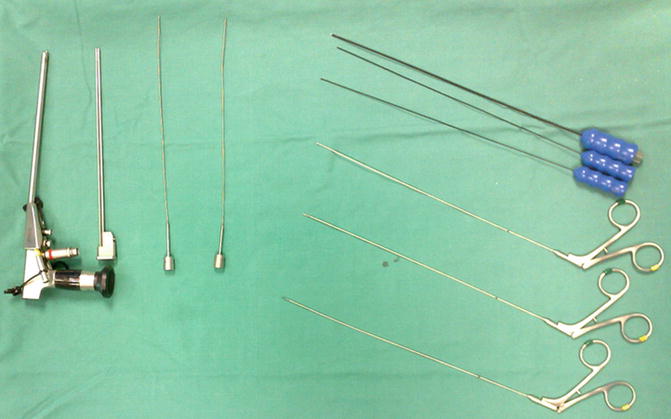
Fig. 7.6
Endoscope system Aesculap MINOP®, shown with its complete instrument set, including obturator, diathermies, biopsy forceps, and scissors (Aesculap AG, Tuttlingen, Germany) (Photograph courtesy of Dr S. Sgouros)
A disposable introducer set (also known as “peel away sheath,” manufactured by several companies) facilitates the process of introducing the endoscope through the brain parenchyma.
Although the neuroendoscopes can be held freehand, there are mechanical and pneumatic holder systems available. For short and straightforward procedures, like an endoscopic third ventriculostomy, they are not necessary, but they can help to facilitate dissection in procedures like intra- and paraventricular tumor removal, when bimanual instrumentation is indicated. Such a holding arm is the Aesculap M-TRAC, which gives both a stable performance (especially for FULL HD cameras) and excellent flexibility and maneuverability for the neuroendoscope. It has an easy mechanical fixation by clamping handle with small, flexible joints for fine positioning and can be used for any surgical intervention when holding of, e.g., optical systems, cameras, instruments, and trocars is needed. Other companies make similar holding arms for their endoscopes.
Other more sophisticated pneumatic systems are also available to hold the endoscope secure during operation. Such a system is the Aesculap UNITRAC®, which is an aid for exact positioning of instruments and video endoscopic systems and for holding retractors in a stable manner over a long period. It is a pneumatic supported system with easy connection to the air supply in the OR with integrated safety systems that prevent collapse of the holding arm if OR compressed air supply is interrupted. It is single-handed in use just by pressing the release button. Other companies make similar pneumatic holding arms for their endoscopes.
The Aesculap NeuroPilot® is a unique steering mechanism for neuroendoscopes offering precise steering of the neuroendoscope by the use of three screws in three dimensions allowing submillimeter maneuvering. After positioning of the neuroendoscope in situ finest corrections or adjustments are often necessary to receive the optimal endoscopic image. With traditional holding devices only a rough positioning is possible; a precise and fine steering of the neuroendoscope is difficult or even not possible.
Altogether, these components allow safe bimanual endoscopic surgery through the endoscope.
For endoscope-controlled procedures like the endoscopic endonasal transphenoidal procedures, dedicated systems have been developed such as the Storz Bettag-Schäfer system with the Thumfart suction-irrigation device (Fig. 7.5) or the Aesculap MINOP® TREND (Fig. 7.7). The MINOP® TREND (TRansnasal ENDoscopy) has a bright 4-mm optic in 0° and 30°. These systems not only are a good to start with transnasal endoscopy but also inspire advanced users to go further and perform extended approaches of the pituitary region and areas of the skull base.

Fig. 7.7
Endoscope system Aesculap MINOP Trend, designed for skull base work (Aesculap AG, Tuttlingen, Germany) (Photograph courtesy of Dr S. Sgouros)
Most surgeons are using a particular system and acquire over the years significant expertise over it. My personal experience with the MINOP® TREND system allows me to say that it is a well-balanced endoscope system offering high ergonomics, a brilliant picture, as well as specially developed instruments. It has an ergonomic handle design and optimum weight distribution, suction, and irrigation that prevents the optic from misting; a revolvable endoscope shaft with angled optics permitting direct visualization of hidden corners of the operating field; and a slim handle for unimpeded panendoscopic manipulation (Fig. 7.8). It can be easily secured to a holding arm.

Fig. 7.8
Bimanual two-hand transnasal endoscopic work, using the Aesculap MINOP Trend system, and a bone drill, during a transnasal transphenoidal operation
One very important component of the whole endoscopic equipment is the camera. Compared to the one-chip cameras used in the 1990s, the present-day’s full high-definition three-chip cameras give excellent views that are indeed comparable to what can be seen through the operating microscope. The full HD camera has a six times higher resolution than conventional standard cameras and delivers crystal clear images of the highest quality (1920 × 1080 pixels). The three-chip technology provides impressive color depth and brilliant red differentiation. The latest Full HD technology delivers lag-free images, even with rapid camera movements. The world’s first 5× zoom in an endoscopy camera shows even the tiniest details in perfect HD quality.
The light source should be a xenon light. Xenon technology achieves a higher efficiency than halogen light sources. It gives extremely high light intensity and excellent color reproduction due to an absolute natural light with a color temperature of 6,000 K (daylight). Special integrated UV filters reduce the highest amount of heat in the visible light.
Related posts:
 Current Status and Future Developments of Neuroendoscopic Management of Pituitary Tumours and Craniopharyngiomas
Current Status and Future Developments of Neuroendoscopic Management of Pituitary Tumours and Craniopharyngiomas
 Endoscopy-Assisted Craniosynostosis Surgery
Endoscopy-Assisted Craniosynostosis Surgery
 Neuroendoscopy in Spinal Pathology: Our Experience, New Trends, and Developments
Neuroendoscopy in Spinal Pathology: Our Experience, New Trends, and Developments
 Neuroendoscopic Treatment of Colloid Cysts
Neuroendoscopic Treatment of Colloid Cysts
 The Application of Neuroendoscopic Techniques in Improving Altered CSF Physiology
The Application of Neuroendoscopic Techniques in Improving Altered CSF Physiology
 Neuroendoscopic Management of Intraparenchymal Lesions
Neuroendoscopic Management of Intraparenchymal Lesions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


