Symptoms
Pre (n patients)
Post (n patients)
% (patient free of symptoms)
Headaches
83
22
73
Visual troubles
34
4
88
Sphincter troubles
8
4
50
Gait and balance troubles
22
5
72
Consciousness troubles
21
3
86
Memory troubles
53
23
56
11.2 Management of Asymptomatic Colloid Cysts
The management of the asymptomatic colloid cysts is still very debatable. Many neurosurgeons advise “prophylactic” surgical removal to avoid catastrophic neurological deterioration. However, long-term follow-up study of 68 subjects with asymptomatic colloid cysts suggests that only a few (8 %) subjects go on to develop symptoms at 10 years [3]. To our opinion asymptomatic cyst should be monitored frequently (at least annually), and patients should be encouraged to report symptomatology without delay. Small (less than 1 cm in diameter) asymptomatic cyst without related hydrocephalus can be managed safely conservatively. If related hydrocephalus is present or the cyst is seen to enlarge on subsequent neuroimaging, risk of deterioration and surgical risk should be balanced, taking into account the clinical condition of the patient and personal preferences.
11.3 Management of Symptomatic Colloid Cysts
The management of symptomatic colloid cysts is always surgical, and the choice of the approach depends on the surgeon’s preferences. Several surgical approaches can be used. The microsurgical transcortical-transventricular and transcallosal approaches were considered gold standard in the days before endoscopy. For the last two decades, the endoscopic approach developed and gained acceptance as an alternative to microsurgical techniques [4–9]. It remains debatable if it can be considered as the preferential and primary surgical modality. Surgical expertise and preference is a dominant factor. During the last decade, a number of series on endoscopic removal appeared [1, 10–18]. Due to the rarity of the disease, most series are relatively small and with limited follow-up. However, many surgeons consider the endoscopic removal of colloid cysts as a valid first-line treatment for these lesions [7, 18–21].
11.4 Neuroendoscopic Technique for Removal of Colloid Cysts
Colloid cysts are the ideal tumors for neuroendoscopic removal except of some limitations (Fig. 11.1): (1) the content of the cyst may be very thick and as a result make the removal difficult [22]; (2) the cyst may be firmly attached to the ventricular walls and the ventricular veins, requiring careful dissection; and (3) a part of the cyst may be hidden under ventricular structures and have a difficult identification.
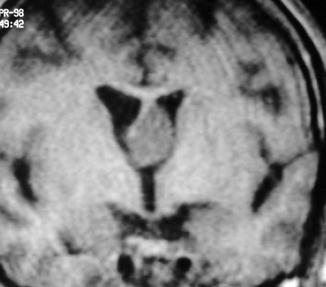
Fig. 11.1
Coronal T1w MR image of a 40-year-old man with persistent headaches. A round mass is seen in the left aspect of the foramen of Monro, causing occlusion of the foramen and unilateral dilatation of the right frontal horn. This is a typical appearance of a colloid cyst
With respect to the operative technique, after general endotracheal anesthesia is administered, the patient is positioned supine. We propose the use of an endoscope that takes large instruments (Fig. 11.2) and offers the possibility of simultaneous use of two instruments (Fig. 11.3) and irrigation (Fig. 11.4) [23]. The neuroendoscope is introduced into the ventricle under freehand guidance. The cyst is approached through a burr hole placed about 4–5 cm lateral to the midline and 1 cm at least (may be more) in front of the coronal suture depending on the ventricular configuration and cyst location. Neuronavigation or stereotactic guidance is only used when the ventricles are small (see Fig. 11.5) [24]. A right-sided approach is chosen unless the cyst is far more prominent through the left foramen of Monro or the right ventricle is too small. The cyst is exposed, coagulated, and punctured and the content aspirated. When possible, the cyst capsule is coagulated at its attachment site, which is then sectioned or carefully pulled out with a forceps to attempt total removal (depends on surgeon’s preference). The use of a supraorbital endoscopic approach to the colloid cysts has been proposed as well, advocating advantages in the visualization of the cyst adhesion to the roof of the third ventricle (Fig. 11.6) [25]. As a surgical advice we would recommend to stay always in the lateral ventricle, avoiding entry into the third ventricle; make safe maneuvering; and always be gentle on grasping and pulling [26].

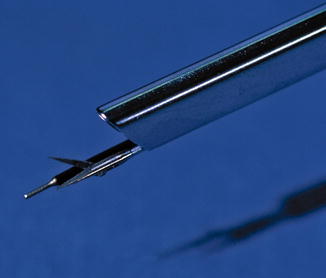

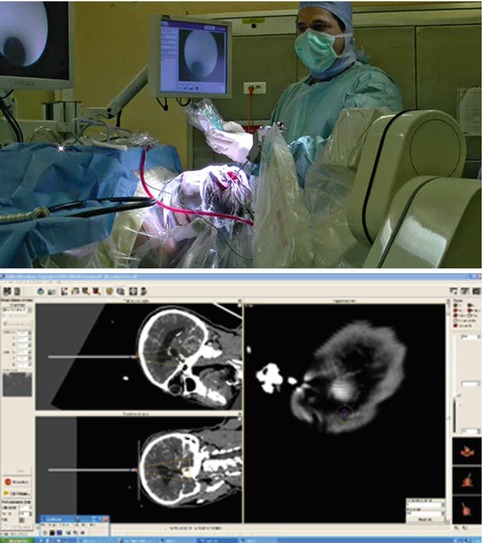
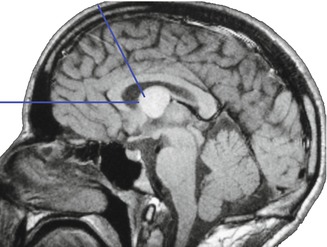
Fig. 11.2
Closeup photograph of the tip of the Storz Decq endoscope, showing the facility to introduce through it a special puncture needle with incorporated aspiration tube. This facilitates the aspiration of the viscous fluid of the colloid cysts
Fig. 11.3
Closeup photograph of the tip of the Storz Decq endoscope, showing the facility to introduce through its two separate working channels a pair of scissors and the monopolar diathermy, simultaneously. This arrangement facilitates greatly the dissection of the cyst capsule from the ventricular walls
Fig. 11.4
Setting of the Storz Decq endoscope with irrigation system
Fig. 11.5
Use of neuronavigation to introduce the endoscope in a small lateral ventricle
Fig. 11.6
Diagrammatic illustration of the endoscopic approaches for removal of colloid cysts, classic and supraorbital, on a sagittal MR image. Directions of surgical approaches (blue lines)
11.5 Results
Recently we published a series of 90 cases between 1994 and 2007 with mean follow-up of 51 months (4, 3 years) [1]. The symptoms can be summarized in Table 11.1, before and after surgery. In this series the Evans’ index improved from 0.42 to 0.36, and only 3 % of the patients needed a permanent shunt. The postoperative result was evaluated with MRI and is divided in three groups radiologically: group A with no remnant visible (Fig. 11.7), group B with remnant membrane or cyst (with CSF), and group C with remnant colloid cyst. The results are shown on Table 11.2 and the complications on Table 11.3. The results are considered good, with high cyst removal rate, low reoperation, and complication rate, comparable if not better to the open craniotomy methods. Certainly, memory disturbance is less following endoscopic removal.
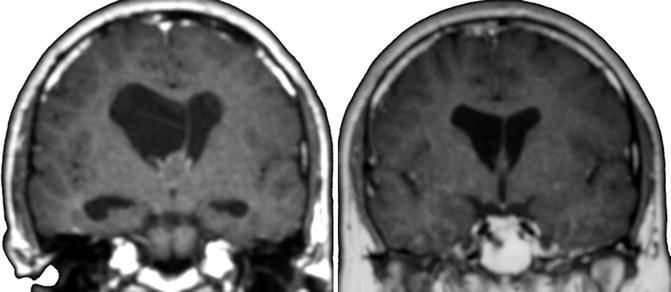
Fig. 11.7
 Neuroendoscopy in Infants and the International Infant Hydrocephalus Study (IIHS)
Historical Trends of Neuroendoscopic Surgery
Endoscopic Endonasal Repair of CSF Leak
Man-to-Machine Interface in Neuroendoscopy: The Importance of Human Interface in the Development of Neuroendoscopy
MRI of Patients with Hydrocephalus
Neuroendoscopic Management of Intraparenchymal Lesions
Neuroendoscopy in Infants and the International Infant Hydrocephalus Study (IIHS)
Historical Trends of Neuroendoscopic Surgery
Endoscopic Endonasal Repair of CSF Leak
Man-to-Machine Interface in Neuroendoscopy: The Importance of Human Interface in the Development of Neuroendoscopy
MRI of Patients with Hydrocephalus
Neuroendoscopic Management of Intraparenchymal Lesions




Preoperative (left) and postoperative (right) coronal T1w MR image of a patient with colloid cyst, which was removed endoscopically
Related posts:
Neuroendoscopy in Infants and the International Infant Hydrocephalus Study (IIHS)
Historical Trends of Neuroendoscopic Surgery
Endoscopic Endonasal Repair of CSF Leak
Man-to-Machine Interface in Neuroendoscopy: The Importance of Human Interface in the Development of Neuroendoscopy
MRI of Patients with Hydrocephalus
Neuroendoscopic Management of Intraparenchymal Lesions
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
