chapter 3
Neurological Examination of the Limbs
Learning how to perform a neurological examination requires repeated practice. Practice without an understanding of how to examine the various aspects of the nervous system and how to interpret the findings is akin to practising golf without having had lessons – useless. This chapter describes how to examine the limbs and interpret the findings. As it is very difficult to learn examination technique from a textbook, a video of the technique is included on the accompanying DVD.
The principal purpose of the examination is to determine whether the patient has lower motor neuron (LMN) signs or, more specifically, signs that indicate involvement of the peripheral nervous system (anterior horn cells, nerve roots, brachial or lumbosacral plexus, peripheral nerve, neuromuscular junction or muscle) or upper motor neuron (UMN) signs that indicate involvement of the central nervous system (brain, cerebellum and spinal cord). These were briefly discussed in Chapter 2, ‘The neurological history’, and, because they are absolutely crucial, they will be discussed in more detail in this chapter (see Table 3.1).
TABLE 3.1
The neurological findings in upper versus lower motor neuron lesions
| Upper motor neuron lesion | Lower motor neuron lesion | |
| Wasting | Usually no wasting but there may be mild wasting with long standing problems | No wasting in the very early stages but usually associated with significant wasting |
| Power | Weakness of extensor muscles in the arms∗ and flexor muscles in the legs∗∗ | The pattern of weakness reflects that part of the LMN that is affected |
| Tone | Increased +/– clonus | Decreased |
| Reflexes | Increased | Decreased or absent |
| Plantars | Up-going (extensor) | Down-going |
| Sensory findings | Sensory level | Focal sensory loss reflecting involvement of a nerve root, plexus or peripheral nerve |
∗Shoulder abduction, elbow extension, wrist and finger extension in the arms.
∗∗Hip flexion, knee flexion and foot dorsiflexion in the legs. The tone may not be increased and the reflexes can be absent in acute spinal cord lesions referred to as spinal shock. Clonus is a series of involuntary repetitive movements of the ankle, up and down, induced by suddenly pushing the foot upwards while the leg is extended [1]. The test is less painful if it is performed with the knee slightly flexed.
THE MOTOR EXAMINATION
The examination of the motor system involves:
• inspecting for wasting and fasciculations in the muscles
• looking for changes in tone and reflexes
Many examiners will perform a screening test of the upper limbs by observing patients elevating their arms and holding them horizontally straight out in front, initially with their eyes open and then subsequently closed (see Figure 3.1). The palms can be turned either down or up – it does not matter – although occasionally having
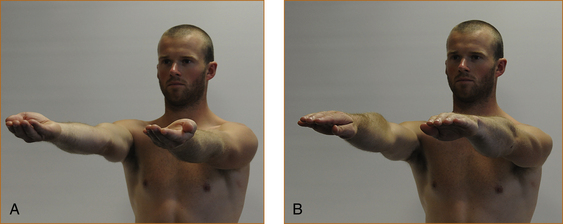
FIGURE 3.1 Screening test of the upper limbs with hands outstretched: A with palms up; B with palms down

• The pathology is always at the level of the LMN signs and at or above the uppermost limit of the UMN signs.
• In most instances the neurological examination does not establish the aetiology or cause of the problem. It simply localises the part of the nervous system that is affected by the pathological process.
• If the history has been obtained using the method described in Chapter 2, ‘The neurological history’, the nature and distribution of the symptoms should provide an idea as to whether there will be upper or lower motor neuron signs.
the palms turned upwards seems a more sensitive technique.1
 If the signs are different, the diagnosis suspected from the history should be reviewed and the whole process should be repeated to confirm both the history and findings. This is far more rewarding than ordering a multitude of purposeless investigations.
If the signs are different, the diagnosis suspected from the history should be reviewed and the whole process should be repeated to confirm both the history and findings. This is far more rewarding than ordering a multitude of purposeless investigations.• drift downwards if there is weakness
• drift upwards and often outwards if there is a proprioceptive or parietal lobe problem
• oscillate up and down with a cerebellar disturbance if the patient is asked to elevate the limbs briskly, which can be missed if the movement is too slow.
Inspection for wasting and fasciculations
The muscles of the upper arm, forearm, hand, thigh, anterior tibial compartment and calves are examined for wasting and/or fasciculations. Fasciculations are visible spontaneous contractions or twitching of muscle fibres that are innervated by a single motor unit [1]. It may be necessary to spend several minutes carefully examining the muscles in order to detect fasciculations. It is easy to be certain that wasting is present when it is very severe, but with milder degrees of wasting one is less certain that there is a lesion involving the peripheral (LMN) nervous system. Some patients are very thin, and inexperienced clinicians may incorrectly suspect wasting when examining the small muscles of the hands, particularly in older patients. If the wasting affects one arm or one leg a comparison can be made with the contralateral limb. The muscles, if wasted, will initially lose their rounded appearance and appear flattened.
The reliable signs of muscle wasting are (Figure 3.2):
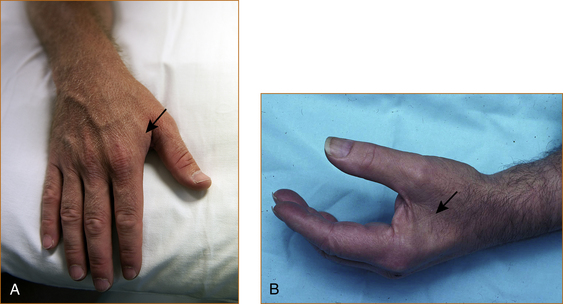
• loss of the visible bulge that occurs when the thumb is adducted towards the index finger – the first dorsal interosseous muscle
• prominence of the anterior border of the tibia – tibialis anterior muscle
• prominence of the spine of the scapula – supraspinatus and infraspinatus muscles
• scalloped appearance just above the patella as if a bite has been taken out of the muscle – quadriceps.
Looking for changes in tone
There are two different ways to test for tone, depending on whether the problem is affecting the motor system or the extrapyramidal system (the latter is discussed in Chapter 13, ‘Abnormal movements and difficulty walking due to central nervous system problems’).
 Tone is tested using quick movements when the motor system is being assessed.
Tone is tested using quick movements when the motor system is being assessed.TESTING FOR INCREASED TONE RELATED TO AN UPPER MOTOR NEURON PROBLEM
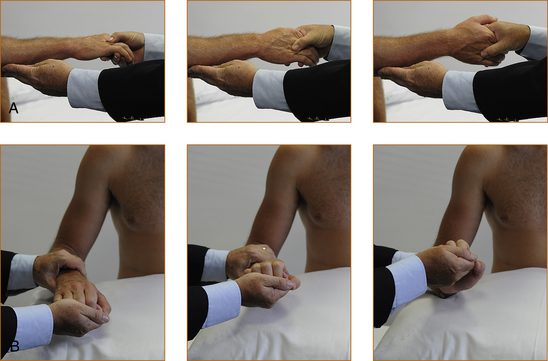
• Arms. Tone is tested with the forearm semi-pronated and the elbow flexed at 90° (refer to Figure 3.3A). The examiner holds the elbow with one hand and then places the other hand in the hand of the patient as if they were shaking hands. The test is performed with a quick supination of the forearm. If there is increased tone there will be a discernible catch. Very occasionally, when the tone is markedly increased, repetitive contractions may occur, and this is referred to as clonus.
• Legs. Tone is tested with the leg lying flat on the bed and slightly externally rotated and with the knee flexed very slightly. The examiner places their hands behind the leg just above the knee and attempts to quickly elevate the leg. If there is increased tone, the heel will lift up off the bed. The leg may lift off the bed in patients who are very anxious and who find it difficult to relax – slight external rotation of the leg prior to the quick movement helps in this situation and eliminates the false impression of increased tone in anxious patients. The other test for increased tone in the legs is ankle clonus, where the leg is slightly flexed at the knee with the ankle plantar-flexed. The examiner places their left hand behind the knee and grasps the foot with their right hand and forcibly dorsiflexes the foot. Repetitive contractions while the examiner holds the foot in dorsiflexion is a sign of increased tone, referred to as ankle clonus.
TESTING FOR INCREASED TONE RELATED TO AN EXTRAPYRAMIDAL PROBLEM
To test the upper limbs (Figure 3.3B), the forearm and hand are pronated and the examiner holds the middle of the forearm with one hand and holds the hand of the patient in a monkey grip. The patient’s hand is compressed into the wrist as the wrist is slowly flexed and extended. This technique will elicit the classical cog-wheel rigidity seen with extrapyramidal problems.
Testing muscle strength
The following technique is recommended when examining muscle strength. The muscle/muscle group, nerve related to that muscle/muscle group, the nerve root(s) and the action of the muscle [2] are listed in each section below. Experienced neurologists have memorised the neuroanatomy; inexperienced clinicians can record the pattern of weakness and consult a textbook of neuroanatomy, the illustrations in Chapter 1, ‘Clinically oriented neuroanatomy’, or this chapter.
UPPER LIMBS
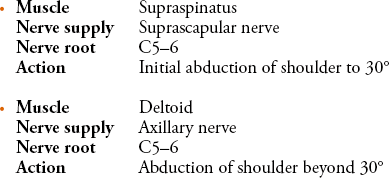
To test the supraspinatus (Figure 3.4) the elbow should be abducted from the side of the body to approximately 30°, the examiner places a hand over the elbow and pushes the elbow towards the trunk while the patient tries to resist.
To test the deltoid muscle (Figure 3.4) the elbow should be abducted from the side to 90°, the examiner places a hand over the upper arm just above the elbow and pushes downwards while the patient attempts to resist.
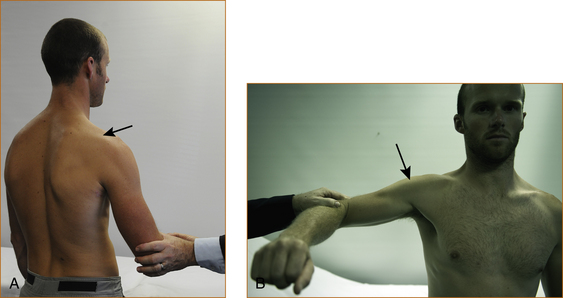
The elbow is kept by the side, the forearm is flexed at 90° and the hand is semi-pronated (Figure 3.5). The examiner places a hand over the middle of the back of the forearm and attempts to internally rotate the forearm towards the body as the patient resists.

The elbow is kept by the side, the forearm is flexed at 90° and the hand is semi-pronated (Figure 3.6). The examiner places a hand on the middle of the forearm and attempts to prevent internal rotation of the forearm.


There is a rare entity of winging of the scapular that is the result of damage to the nerve to the serratus anterior (see Chapter 11, ‘Common neck, arm and upper back problems’). The patient is instructed to stand in front of a wall, with the elbows slightly flexed and the palms on the wall (Figure 3.7). They are then instructed to push as hard as they can and the scapular should not lift off the chest wall. If it does the muscle is weak, resulting in ‘winging of the scapula’.

The elbow is bent at 90° with the palm pointing towards the ceiling (Figure 3.8). The examiner grasps the elbow with the left hand and the wrist with the right hand and attempts to prevent further flexion of the elbow.


The elbow is flexed at 90° with the forearm semi-pronated (Figure 3.9). The examiner places the left hand under the elbow and the right hand on the wrist and attempts to prevent further flexion of the elbow.

FIGURE 3.9 Testing elbow flexion with the forearm semi-pronated
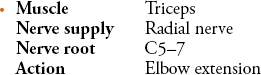
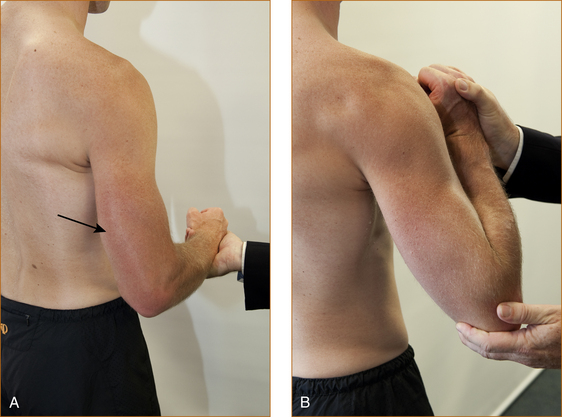
It is very important that the elbow is only slightly flexed (as little as 20–30° from the fully extended position) when testing extension (Figure 3.10). If the elbow is fully flexed, this will result in an apparent weakness of the triceps when it is strong and, if it is fully extended, subtle degrees of weakness may be missed. The examiner places the left hand over the anterior aspect of the elbow and the right hand over the dorsal aspect of the wrist and attempts to prevent the patient from straightening their elbow.

Related posts:
 AFTER THE HISTORY AND EXAMINATION, WHAT NEXT?
AFTER THE HISTORY AND EXAMINATION, WHAT NEXT?
 ABNORMAL MOVEMENTS AND DIFFICULTY WALKING DUE TO CENTRAL NERVOUS SYSTEM PROBLEMS
ABNORMAL MOVEMENTS AND DIFFICULTY WALKING DUE TO CENTRAL NERVOUS SYSTEM PROBLEMS
 COMMON NECK, ARM AND UPPER BACK PROBLEMS
COMMON NECK, ARM AND UPPER BACK PROBLEMS
 CLINICALLY ORIENTED NEUROANATOMY: ‘MERIDIANS OF LONGITUDE AND PARALLELS OF LATITUDE’
CLINICALLY ORIENTED NEUROANATOMY: ‘MERIDIANS OF LONGITUDE AND PARALLELS OF LATITUDE’
 THE CRANIAL NERVES AND UNDERSTANDING THE BRAINSTEM THE ‘RULE OF 4’
THE CRANIAL NERVES AND UNDERSTANDING THE BRAINSTEM THE ‘RULE OF 4’
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


