CHAPTER 120 NEUROLOGY OF PULMONOLOGY AND ACIDBASE DISTURBANCE
Respiration is essential for cellular metabolism, and no other organ is more dependent on oxygen supply than is the brain. The consequences of disturbances in gas exchange are readily reflected in disturbance of neuronal function, in neuronal injury, or in death. The respiratory system is crucial for the gas exchange and plays a large part in acidbase homeostasis. Neuronal integrity and respiratory regulation are highly interdependent. A brief conceptualization of the neurological control of breathing is necessary for understanding various disordered respiratory patterns. Clinical respiratory abnormalities can be viewed in three contexts: disturbances in the neural control of respiration, in the respiratory apparatus, or in the carriage or composition of blood gases. This chapter describes abnormalities associated with neurological control of respiration and neurological consequences of respiratory dysfunction.
NEURAL CONTROL OF RESPIRATION
The nervous system is intricately connected to the mechanics of respiration at various levels. From the cerebral cortex via the brainstem to the level of the lower motor neurons, the nervous system regulates respiratory effort. It is aided by feedback from peripheral chemoreceptors and mechanoreceptors (Fig. 120-1).1 The anterior horn cells controlling respiratory muscles represent the lower motor neurons, which control the actual mechanics of breathing. Inspiratory muscles generate subatmospheric pressures within the thorax and induce airflow and gas exchange at the alveolar level.
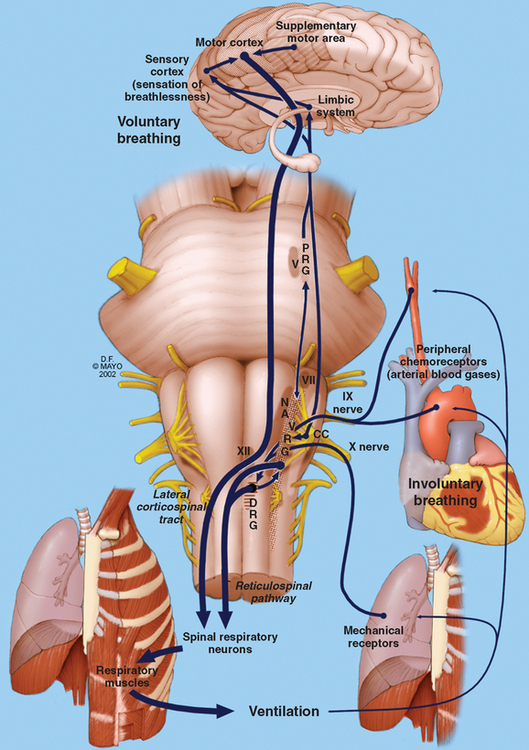
Lower Motor Components of Respiration
The lower motor components are composed of neurons innervating the diaphragm, intercostal muscles, abdominal muscles, and other accessory muscles.1 During quiet breathing, only the diaphragm is vigorously active, with some contribution from the abdominal and external intercostal muscles. These muscles work in conjunction with muscles of the upper airway to maintain a patent airway and ensure an uninterrupted passage to air. The diaphragm is the most important inspiratory muscle, and it derives its nerve supply via the phrenic nerve from spinal cord segments C3-C5. Other inspiratory muscles include the external intercostal muscles, the parasternal intercostal muscles, and the scalene muscles.
Upper airway structures are crucial in maintaining the patency of airways. Dysfunction of these structures is readily evident in abnormalities of speech and swallowing, as well as in obstructive sleep apneas and other breathing disorders. The muscles of the nose, mouth, soft palate, pharynx, epiglottis, and larynx work in conjunction to ensure a free flow of air into the trachea and bronchi. Somatic innervation of these muscles is provided by the lower cranial nerves: V, VII, IX, X, and XII.
ABNORMAL RESPIRATORY PATTERNS IN NEUROLOGICAL DISEASES
Respiratory Failure
Neurological disorders can produce dyspnea or frank respiratory failure. Respiratory failure exists when arterial oxygen tension (PaO2) is less than 60 mmHg or when PaCO2 exceeds 50 mmHg when the patient is breathing air, and it is the end result of respiratory dysfunction. It can exist in acute and chronic forms. Acute respiratory failure manifests dramatically, and most patients are immediately intubated and ventilated. Nearly 300,000 cases of acute respiratory failure are encountered each year in the United States; the approximate incidence is 137 cases per 100,000 population.2 The number of cases related to neurological disorders is not known. Nevertheless, even if it is assumed that only 0.5% to 1% of cases of acute respiratory failure are related to neurological causes, they add up to 1500 to 3000 cases per year in the United States alone.
In clinical practice, the neurologist is most often consulted about patients with respiratory failure in which a clear pulmonary or medical cause is not evident. Sometimes the neurologist is consulted when there is difficulty in weaning a patient from a ventilator. This is common in the intensive care unit with critically ill patients who may display a necrotizing myopathy.3 Alternatively, respiratory failure may supervene in patients with known neurological illness such as myasthenia gravis or Guillain-Barré syndrome. Examination reveals tachypnea, brow sweating, tachycardia, weak cough, paradoxical respiration, and diminished respiratory muscle strength on pulmonary function tests. Patients with chronic respiratory failure may present with an insidious onset of sensorial alteration and coma. The commonest neurological causes of respiratory failure are neuromuscular and spinal cord disorders.4 Peripheral disorders result in respiratory muscle weakness, alveolar hypoventilation, and type II respiratory failure. Table 120-1 lists some of the common neuromuscular and spinal disorders producing respiratory weakness. Most of these disorders can manifest with acute or chronic respiratory failure. Associated findings, pulmonary function test results, neurophysiological evaluation findings, and muscle/nerve biopsy findings help identify most of these peripheral or spinal causes of respiratory failure.
TABLE 120-1 Neuromuscular Conditions Resulting in Respiratory Failure
< div class='tao-gold-member'> Only gold members can continue reading. Log In or Register to continue
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
